







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Erectile dysfunction — the inability to get or keep an erection firm enough for sex — affects more men than almost any other treatable condition. Around 40% of men over 40 and 70% over 70 experience some form of ED, and younger men are increasingly affected too. The good news: after four decades of research, an effective treatment now exists for the vast majority of cases — it’s often a matter of finding the right one.
This is a complete, evidence-based erectile dysfunction treatment guide for 2026. You’ll learn what ED actually is, the underlying causes (from blocked arteries to stress), how doctors diagnose it, every modern treatment option from lifestyle to surgery, how the major PDE5 inhibitors compare, and what to do when the first thing you try doesn’t work. No judgement, no hype — just the clinical science that drives current practice.
- ED is almost always multifactorial — a mix of vascular, hormonal, neurological and psychological contributors.
- The oral PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil) are first-line medical therapy, effective in roughly 70% of men.
- Lifestyle changes — exercise, weight loss, smoking cessation, Mediterranean-style diet, sleep — produce effects comparable to pills and should always be part of the plan.
- ED is often the earliest warning sign of underlying cardiovascular disease, sometimes 3-5 years before a heart attack. It is worth a proper check-up.
- If pills don’t work, newer options — intra-cavernosal injection, vacuum devices, low-intensity shockwave therapy, penile implant — solve more than 95% of remaining cases.
- Talking to a doctor early works better than hoping it resolves on its own. Most treatments work; the hardest step is the first one.
What Is Erectile Dysfunction?
Quick Answer: What is ED?
Erectile dysfunction is the persistent inability to achieve or maintain an erection firm enough for satisfactory sexual activity, for at least three months. Occasional difficulties are normal — ED is about pattern and duration, not one-off events. It is treatable in roughly 95% of men, and the first-line treatment is oral medication combined with lifestyle change.
An erection is a vascular event. Arousal signals from the brain travel down the spinal cord and dilate the arteries that feed the penis. Blood fills two sponge-like chambers called the corpora cavernosa, which expand and compress the veins that normally drain the penis — holding the erection in place until arousal subsides.
ED occurs when any part of this sequence fails. Blood may not get in (vascular problem), signals may not arrive (neurological), the trigger hormones may be missing (hormonal), or anxiety and psychological factors override arousal (psychogenic). In about two-thirds of men with ED, more than one cause is involved.
The clinical definition (DSM-5 and urology guidelines) requires difficulty on at least half of attempts, for at least three months, causing distress or relationship impact. One-off or situational problems — tiredness, alcohol, unfamiliar partner — don’t count as ED. A consistent pattern, especially one that gets worse, does.
How Common Is ED?
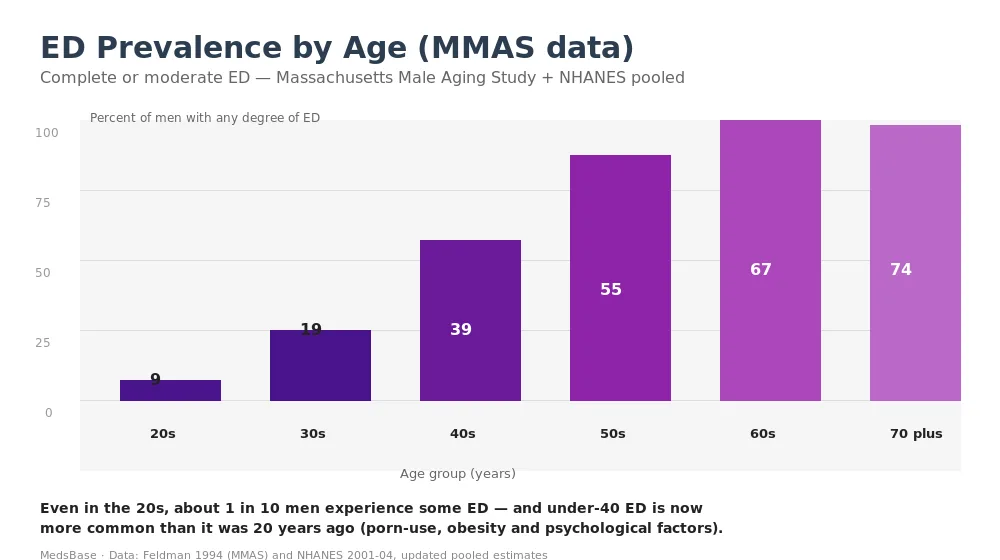
The Massachusetts Male Aging Study (MMAS, Feldman 1994), NHANES, and a series of later global surveys converge on a consistent pattern: ED risk rises roughly 10 percentage points per decade of life. By the mid-40s, nearly 4 in 10 men have some degree of ED. Over 70, close to 3 in 4 are affected.
Under-40 ED is rising. Surveys from the last decade suggest prevalence in men in their 20s has increased from around 2-5% historically to 9-15% today. Likely drivers: rising obesity rates, higher anxiety and depression prevalence, increased use of antidepressants (which can reduce libido and orgasm function), and — more controversially — high pornography use reshaping arousal patterns.
Despite how common ED is, only about 25% of men with the condition seek medical help. That reluctance often costs years of unnecessary suffering — most cases resolve well once they enter the treatment pipeline.
What Causes Erectile Dysfunction?
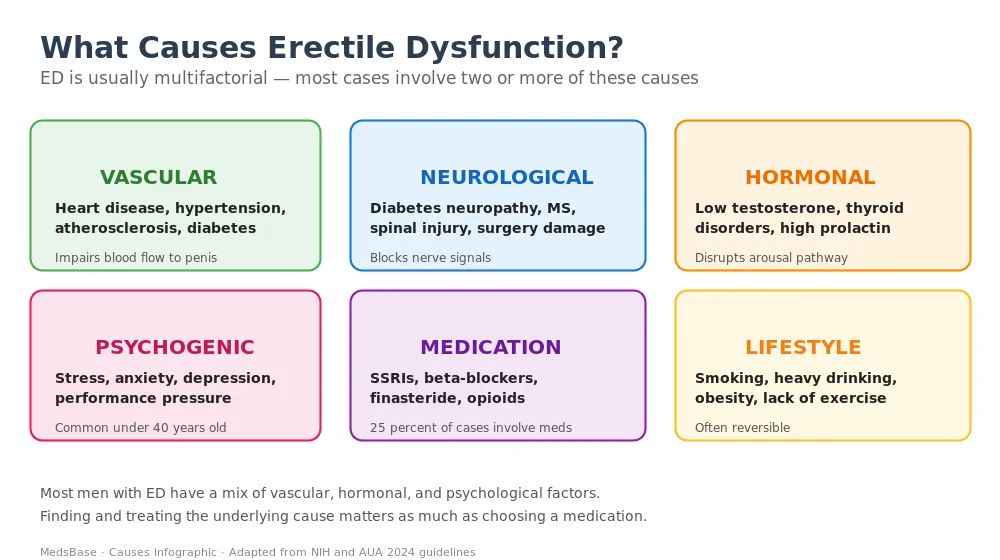
Vascular (most common)
The same processes that narrow arteries feeding the heart — atherosclerosis, high blood pressure, diabetes, high cholesterol — also narrow the small arteries feeding the penis. Because penile arteries are narrower to begin with (~1-2 mm diameter, vs 3-4 mm for coronaries), they show damage first.
This is why ED is often called a “canary in the coal mine” for cardiovascular disease. A 2013 meta-analysis showed men with new-onset ED had a 43% increased risk of a cardiovascular event within the next 7-10 years — meaningful enough that all men presenting with unexplained ED should have basic cardiac risk assessment.
Neurological
Diabetes (even well-controlled) causes small-nerve damage that impairs the autonomic signals driving erection. Multiple sclerosis, Parkinson’s disease, spinal cord injury, and the after-effects of prostate or pelvic surgery can all disrupt the same pathway. The pattern is usually gradual progression, often with other sensory symptoms in hands or feet.
Hormonal
Low testosterone (hypogonadism) reduces libido, morning erections, and arousal. True hypogonadism (measured morning testosterone under 300 ng/dL combined with symptoms) affects about 2-5% of men under 50 and 10-20% over 60. Thyroid disorders (both over- and under-active) and hyperprolactinaemia are less common but treatable contributors.
Psychogenic
Performance anxiety, depression, relationship stress, and post-traumatic responses can all suppress arousal pathways. Psychogenic ED is more common in men under 40 and is often signalled by preserved morning and masturbatory erections (the machinery works — the context is the problem). It responds best to a combination of pills and talking therapy.
Medication-induced
About 1 in 4 ED cases involve a contributing medication. The biggest offenders: beta-blockers (except nebivolol), thiazide diuretics, SSRIs, finasteride and dutasteride, opioids, and older antihistamines. Never stop a prescribed drug on your own — ask the prescriber whether a switch is possible.
Lifestyle
Smoking, heavy drinking (over 14 units/week), obesity, poor sleep, and a sedentary routine all contribute. These are also the most reversible — many men see meaningful improvement from lifestyle change alone, without any medication. See our full guide on weight loss and ED for the specific mechanisms.
How Is ED Diagnosed?
A competent ED work-up is usually 80% history-taking. Your doctor will ask about the pattern of symptoms, medications, alcohol and recreational drug use, relationship context, and any existing medical conditions. A focused physical exam assesses blood pressure, body-mass index, penile and testicular anatomy, secondary sex characteristics, and sometimes the cardiovascular exam.
Routine investigations typically include fasting glucose and HbA1c, a lipid profile, morning total testosterone (ideally 8-10 AM, on two separate occasions if low), free testosterone if total is borderline, LH, FSH, prolactin, and thyroid function. For men over 50 or with risk factors, a cardiac risk assessment is worthwhile — the European Society of Cardiology recommends ECG and sometimes exercise testing before prescribing PDE5 inhibitors to men with cardiac risk.
The International Index of Erectile Function (IIEF-5) is a five-question validated questionnaire used to stratify severity:
- 22-25: No ED
- 17-21: Mild ED
- 12-16: Mild-to-moderate ED
- 8-11: Moderate ED
- 1-7: Severe ED
Repeating it after treatment is the simplest way to tell if a medication or lifestyle change is working.
Treatment Options Overview
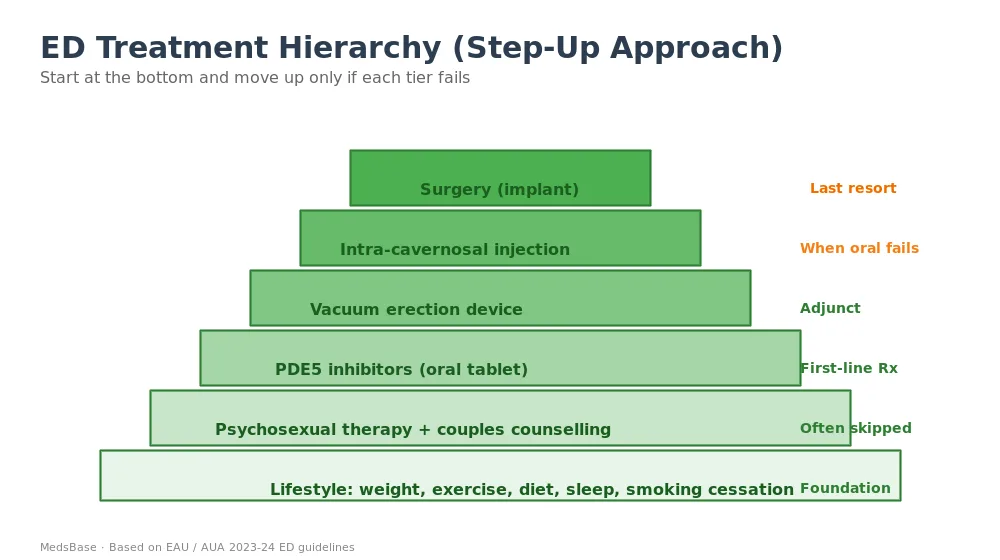
Modern ED care follows a step-up model. Start at the base of the pyramid and escalate only if each tier proves insufficient. The tiers are:
- Lifestyle foundation: weight, exercise, diet, sleep, smoking cessation, alcohol moderation — always, at every stage.
- Psychosexual therapy: often skipped but dramatically effective, especially in psychogenic or mixed-cause cases.
- Oral PDE5 inhibitors (first-line drug therapy): sildenafil, tadalafil, vardenafil, avanafil.
- Adjunct: vacuum erection device (VED) — useful especially after surgery or when pills partially work.
- When oral fails: intra-cavernosal injection or intra-urethral alprostadil.
- Last resort: penile prosthesis implant surgery. Success rate >95% but irreversible.
Most men never need to leave tiers 1-3. The right medical plan combines lifestyle change + one first-line medication, reassessed every 6-12 weeks.
PDE5 Inhibitors — The First-Line Medication
PDE5 inhibitors (phosphodiesterase type 5 inhibitors) work by preventing the breakdown of cyclic GMP — the molecule that keeps penile blood vessels relaxed and open during arousal. They don’t cause an erection. They remove the brake that was preventing one. Sexual stimulation is still required.
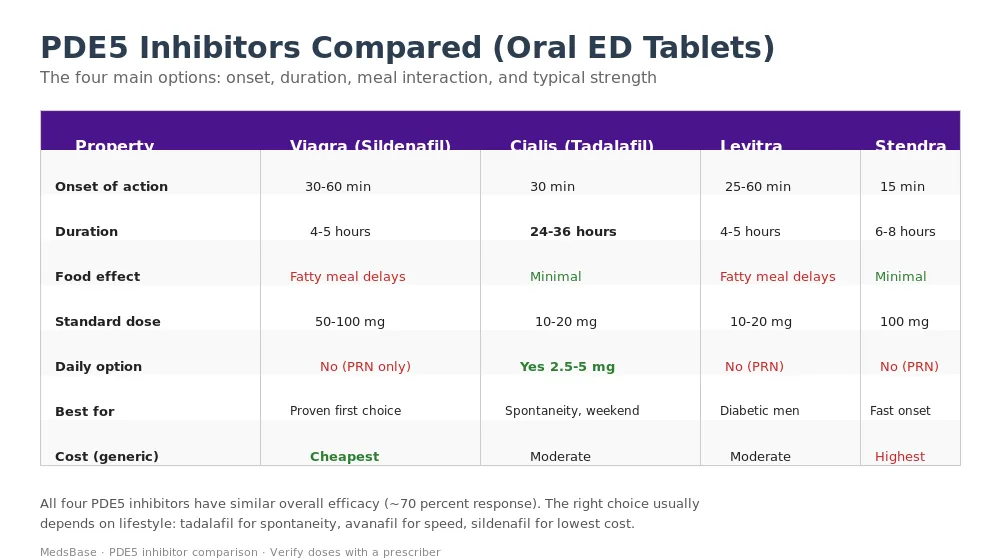
Overall response rate across the four approved agents is similar, around 70%. Differences between them are practical: speed of onset, how long they last, and whether food (especially fat) blunts absorption.
Sildenafil (Viagra, Suhagra, Cenforce, Kamagra)
The original. FDA-approved 1998. Onset 30-60 minutes, duration 4-5 hours. Fatty meals delay absorption. Starting dose 50 mg, range 25-100 mg. Now widely available generically — often the cheapest choice and the benchmark everything else is compared to. Browse our Suhagra 100 mg guide or Viagra Jelly 100mg for the liquid formulation.
Tadalafil (Cialis, Tadarise)
Known as the “weekend pill.” Onset 30 minutes, duration 24-36 hours. Minimal food interaction. Uniquely available as a low-dose once-daily option (2.5-5 mg) that keeps blood levels steady, so erections are possible at any point without planning. Often preferred by men with BPH symptoms — also treats those.
Vardenafil (Levitra)
Onset 25-60 minutes, duration 4-5 hours. Some evidence of better response in diabetic men, though meta-analyses are mixed. Fatty meals delay absorption. Generally interchangeable with sildenafil for most users.
Avanafil (Stendra)
Newer and faster. Onset 15 minutes, duration 6-8 hours, minimal food interaction. Typically the most expensive option because patent protection has lasted longer.
What if the first PDE5 inhibitor doesn’t work?
A third of first prescriptions fail at the starting dose. Before concluding “PDE5 inhibitors don’t work for me,” try:
- Maximum licensed dose (100 mg sildenafil, 20 mg tadalafil) on at least 4 separate attempts
- Take on an empty stomach or with a low-fat meal
- Allow a full hour of waiting (especially for sildenafil/vardenafil)
- Ensure adequate sexual stimulation — it is not an aphrodisiac
- Switch to a different PDE5 inhibitor if the first fails — about half of non-responders respond to an alternative
- Combine with daily low-dose tadalafil to reinforce baseline vascular tone
Side effects and safety
PDE5 inhibitors are safe for the great majority of men. The commonest side effects are headache (15%), flushing (10%), nasal congestion (5%), indigestion (5%), and blue-tinged vision (2%, mostly sildenafil). Rare but serious concerns: priapism (erection over 4 hours — seek urgent care), sudden hearing loss, and NAION (an eye complication).
Absolute contraindications include use with any nitrate drug (causes dangerous blood pressure drop), within 90 days of heart attack, severe hypotension or uncontrolled hypertension, recent stroke, or severe hepatic impairment.
Other Medical Treatments
Alprostadil (injection or urethral pellet)
Alprostadil is a direct vasodilator delivered either as a self-injection into the base of the penis or as a small pellet inserted into the urethra. Response rate is around 85%, including many men in whom PDE5 inhibitors fail. The injection (Caverject, Invicorp) is more reliable but understandably intimidating — most men need careful training with a urology nurse before using at home.
Testosterone replacement therapy (TRT)
If blood testing confirms low testosterone with symptoms, TRT (gel, injection, or pellet) may improve libido, energy, and erection quality. It is not a first-line ED treatment in men with normal levels — supplementation in eugonadal men provides no benefit and may cause harm. Expect 3-6 months before full effect, and ongoing monitoring of haematocrit, PSA, and symptoms.
Vacuum erection device (VED)
A mechanical pump that draws blood into the penis; a constriction ring is then placed at the base to hold the erection for up to 30 minutes. Reliable, cheap, and drug-free. Often combined with PDE5 inhibitors or used during rehabilitation after prostatectomy.
Low-intensity shockwave therapy (Li-ESWT)
Still emerging. Small studies suggest repeated sessions stimulate new blood vessel growth in the penis. Response rates and durability remain uncertain, and insurance coverage is rare. Reasonable to consider in carefully selected patients with mild-to-moderate vasculogenic ED.
Penile prosthesis (implant surgery)
A two-piece or three-piece inflatable device placed surgically inside the corpora cavernosa. Used when every other option has failed. Satisfaction rates >90% — one of the highest in all of urology — but the procedure is irreversible and removes any residual natural erection capacity.
Lifestyle Interventions — More Powerful Than People Realise
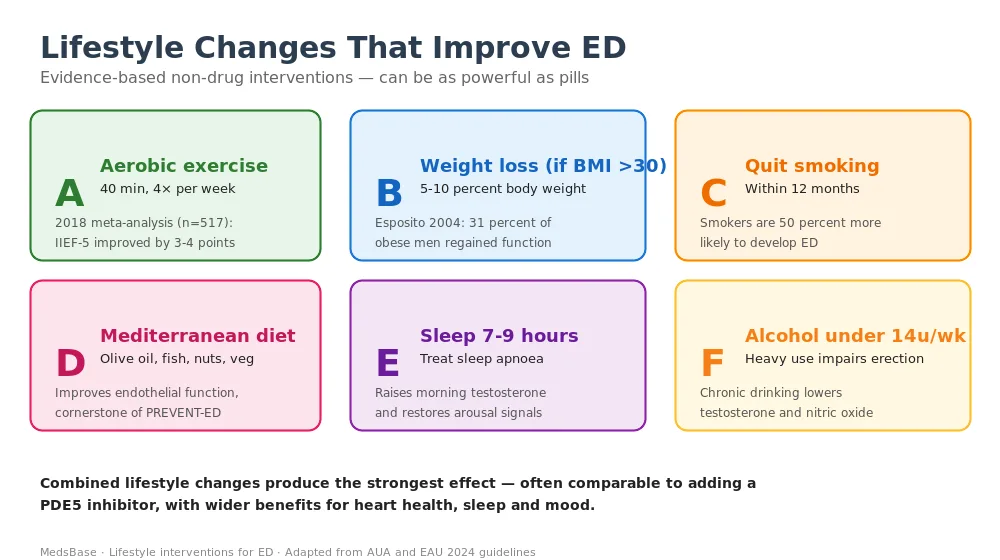
Aerobic exercise
A 2018 meta-analysis of 517 men across 7 randomised trials found aerobic exercise (4 sessions/week, 40 minutes, moderate intensity) improved IIEF scores by 3-4 points — comparable to starting a PDE5 inhibitor. Running, swimming, brisk walking, cycling (on upright rather than narrow saddles): all work. Pelvic-floor physiotherapy adds further benefit.
Weight loss
In obese men, 5-10% body weight loss produces measurable improvement. The Esposito et al. 2004 trial in JAMA randomised obese men with ED to a Mediterranean diet + exercise or standard advice — at 2 years, 31% of the intervention group no longer met ED criteria, vs 5% of controls. Newer GLP-1 agonists like tirzepatide and semaglutide now make weight loss achievable for many men who previously couldn’t — with parallel improvements in erectile function.
Smoking cessation
Smokers have a 50% higher risk of developing ED. Quitting reverses much of that risk within 1-2 years. Nicotine replacement (patches, gum, lozenges) or prescription aids (bupropion, varenicline) double quit rates compared to willpower alone.
Mediterranean-style diet
Rich in olive oil, vegetables, legumes, nuts, fish, and whole grains. Low in processed meat, refined carbohydrates, and sugar. Improves endothelial function — the same vascular bed that erections depend on. The PREDIMED trial associated the diet with significantly lower ED incidence.
Sleep (7-9 hours, treat apnoea)
Obstructive sleep apnoea is a hidden ED cause. Intermittent overnight hypoxia suppresses testosterone and damages vasculature. CPAP therapy restores erectile function in most men with severe OSA and ED, often within 6 months. If you snore heavily, wake unrefreshed, or have witnessed apnoeas, ask for a sleep study.
Alcohol moderation
Heavy drinking both impairs erection acutely and damages nerves and hormones long-term. Keeping intake under 14 units/week (UK guideline) minimises risk.
Natural supplements — what the evidence shows
A handful of supplements have modest evidence. L-arginine (5-6 g/day) improves vascular function in some studies. L-citrulline converts to arginine. Panax ginseng shows small effect in meta-analyses. Our horny goat weed vs Viagra comparison looks at one of the better-studied herbal options. Supplements are less effective than PDE5 inhibitors but can suit men with mild ED or who prefer to start without a prescription.
Psychological and Relationship Treatments
Psychological factors contribute to roughly 10-20% of ED cases as the sole driver, and to about half of all cases as a partial cause. Addressing these is often the missing piece.
Cognitive behavioural therapy (CBT) for sexual performance anxiety breaks the worry-failure-avoidance cycle. A brief course (6-10 sessions) often produces lasting improvement.
Sex therapy or couples counselling addresses relationship dynamics, communication, and sexual technique. Dramatic changes happen when both partners work together — and when the problem stops being “his fault.”
Treating depression and anxiety with appropriate non-ED-worsening medication (bupropion, mirtazapine, and newer options rather than SSRIs when possible) can restore function alongside mood.
Many men benefit from combining a PDE5 inhibitor with brief therapy — pills handle the immediate event; therapy treats the context. After 3-6 months of success, some men can wean off medication entirely.
How to Choose the Right Treatment
A sensible starting plan for most men with mild-to-moderate ED looks like this:
- Confirm the diagnosis with a doctor — including basic blood work and cardiac risk review.
- Address the lifestyle fundamentals: weight, exercise, smoking, alcohol, sleep. Expect 8-12 weeks before you see effect.
- Try a low-dose sildenafil or tadalafil depending on whether you want on-demand or spontaneity.
- Reassess at 6-12 weeks using an IIEF-5 score. If effect is inadequate, increase dose or switch agent.
- Add brief therapy if there’s a relationship or psychological component.
- Escalate to alprostadil, VED, or surgical consultation only after PDE5 inhibitors have genuinely failed at maximum dose with good technique.
Almost every man who follows this sequence patiently ends up at a workable result. The hardest step is usually the first — having the conversation.
You can browse our full sexual health product range at MedsBase, which includes sildenafil, tadalafil, vardenafil, and avanafil in multiple strengths and formulations.
Frequently Asked Questions
Is erectile dysfunction curable?
Many cases are curable, not just treatable. Lifestyle-driven and psychogenic ED often resolves completely with weight loss, exercise, smoking cessation, and therapy. Hormonal ED resolves when the underlying cause is corrected. Vascular ED tends to require ongoing treatment but responds very well to PDE5 inhibitors in most men. Overall, 95% of men get back to satisfying sexual function with current options.
What is the most effective treatment for ED?
The most effective first-line treatment is an oral PDE5 inhibitor combined with lifestyle change — producing response in about 70% of men. For men who don’t respond, intra-cavernosal alprostadil injection works in 85%, and penile prosthesis implant surgery has >95% success. Effectiveness depends heavily on matching the right tool to the underlying cause.
Can erectile dysfunction be a sign of something serious?
Yes. ED can be an early sign of cardiovascular disease, diabetes, low testosterone, or depression — sometimes appearing 3-5 years before a heart attack. Any man with new unexplained ED should have blood pressure, fasting glucose, cholesterol, and testosterone checked. Treating ED without checking for these underlying drivers misses a significant preventive opportunity.
How quickly does Viagra or Cialis start working?
Sildenafil (Viagra) typically works in 30-60 minutes, peaking at 1 hour. Tadalafil (Cialis) works in about 30 minutes and lasts up to 36 hours. Avanafil (Stendra) is the fastest at 15 minutes. Food — especially fatty meals — delays sildenafil and vardenafil by up to two hours; tadalafil and avanafil are far less affected. Sexual stimulation is required in all cases.
Are there natural remedies that actually work?
A few have modest evidence: L-arginine or L-citrulline (5-6 g/day), Panax ginseng, and horny goat weed (icariin) all show small benefit in small trials. None approach the reliability of PDE5 inhibitors. They are reasonable to try for mild ED or as an opener before seeing a doctor. Quality control in over-the-counter supplements is variable — use reputable brands and avoid proprietary “male enhancement” blends.
Can ED medications damage my heart?
For men without nitrate medication or very advanced heart disease, PDE5 inhibitors are cardiovascularly safe — they do not cause heart attacks. The statistical association between ED drug use and cardiac events in older data reflects underlying cardiac risk, not the drug itself. The combination that is genuinely dangerous is any PDE5 inhibitor with any nitrate (GTN spray, isosorbide tablets) — that can cause a fatal blood pressure collapse.
Will ED go away on its own?
Lifestyle-driven and situational ED often improves on its own when the trigger resolves (stress passes, relationship improves, sleep returns to normal). Age-related vascular ED rarely reverses without treatment. Waiting more than 3-6 months before seeking help is almost always a mistake — earlier treatment is easier, and many underlying causes (diabetes, heart disease) benefit from being caught early.
What’s the difference between ED and low libido?
ED is a problem with the physical erection — desire is present but the response fails. Low libido is absent or markedly reduced sexual desire. They can occur together, especially when testosterone is low. Treating one doesn’t automatically treat the other: PDE5 inhibitors restore erections but don’t raise libido, and testosterone therapy raises libido but may not restore erections alone.
Is it safe to buy ED medication online?
It can be — provided you buy from a regulated pharmacy that requires a prescription (or includes an online clinician consultation) and dispenses licensed medication. Avoid websites that sell without any prescription check, make unrealistic claims, or offer unbranded “generic blue pills” at extreme discounts — counterfeit ED medication is one of the most common classes of fake drug worldwide.
The Bottom Line
Erectile dysfunction is one of the most treatable conditions in medicine — and one of the least talked about. The evidence is clear: the great majority of men get back to satisfying sexual function with some mix of lifestyle change, psychological support, and first-line PDE5 inhibitors. When those don’t work, newer medical and surgical options solve almost every remaining case.
The practical playbook for 2026: don’t wait. Talk to a doctor early, get a basic blood work-up, address any underlying cardiovascular or hormonal drivers, start on lifestyle changes, and try a low-dose PDE5 inhibitor. Reassess at 12 weeks. Escalate only if needed.
If you’re considering a medical option, you can explore our full sexual health catalogue at MedsBase — including sildenafil-based (Cenforce, Suhagra, Kamagra), tadalafil-based, and vardenafil-based options in multiple strengths. For related reading, see our Horny Goat Weed vs Viagra comparison, Can weight loss treat ED?, What causes erectile dysfunction?, and How to make ED medication work better.
Last updated: 2026-04-17 · Reviewed by MedsBase Clinical Content Team.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.