







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

Reviewed by the MedsBase Editorial Team · Last updated: April 17, 2026
Roughly 50% of men experience noticeable male-pattern baldness by age 50, and about 40% of women experience some degree of female-pattern hair thinning by the same age, according to the American Academy of Dermatology. If you’ve started researching treatment, you’ve almost certainly seen minoxidil 5% vs 10% come up as a recurring question — especially on forums and specialist sites that sell the higher concentration that mainstream pharmacies don’t stock.
The assumption most people make: if 5% works, 10% must work twice as well. The reality, from the clinical trial data, is more complicated. Higher-strength minoxidil does deliver measurably more hair growth in some patients — but the size of that extra benefit is smaller than most people expect, and the side-effect profile climbs in step. This guide walks through exactly how much extra benefit you actually get, who should consider moving up from 5%, and who should stay put.
- Minoxidil 5% is the FDA-approved gold-standard for male and female pattern hair loss.
- Minoxidil 10% is not FDA-approved; it’s sold through compounding pharmacies and specialty markets (including Indian generics).
- Head-to-head studies show ~15–20% additional hair-count gain with 10% over 5% — but with significantly more scalp irritation.
- 10% minoxidil is generally not recommended for women because of increased facial hypertrichosis risk.
- Both concentrations take 3–6 months to show visible results and must be used continuously to maintain them.
- Low-dose oral minoxidil has emerged as a parallel option for patients who can’t tolerate topical formulations.
Minoxidil 5% vs 10% — Is the Stronger Concentration Actually Better for Hair Loss?
What Is Minoxidil?
Quick Answer — What is Minoxidil 5% vs 10%?
Minoxidil is a topical (and sometimes oral) hair-loss treatment originally developed as a blood pressure drug in the 1970s. Hair regrowth emerged as a systemic side effect, which led to its FDA approval as a topical therapy in 1988. Today it’s the most widely used treatment for androgenetic alopecia (male- and female-pattern hair loss), typically applied twice daily to the scalp as a 2%, 5%, or off-label 10% solution or foam.
Minoxidil was originally developed by the Upjohn Company (now Pfizer) as an oral antihypertensive drug called Loniten. During clinical trials, researchers noticed an unusual side effect: patients were growing more body and scalp hair. That discovery triggered a development program for a topical formulation, which led to the 1988 FDA approval of Rogaine 2% for men with male-pattern baldness. The 5% concentration followed, and in 2014 the 5% foam was also approved for women.
Outside the US, minoxidil is sold under many names: Tugain (Cipla), Mintop (Dr Reddy’s), Minoxytop, Regaine, and dozens more. Indian generic manufacturers have also produced 10%, 12%, and even 15% concentrations — usually marketed to men who have plateaued on 5% and want more aggressive regrowth. Those higher strengths are not FDA-approved in the US.
On MedsBase, minoxidil products include Minoxytop (Minoxidil), Tugain Foam, Tugain Solution, Regaine 5%, Mintop Lotion, and oral Lonitab.
Why there’s demand for higher-strength minoxidil
For most men, 5% delivers meaningful regrowth — but not for everyone. Studies show that roughly 30–40% of users are “non-responders” to standard 5%, either because of low activity of the scalp enzyme that activates minoxidil (SULT1A1), genetic differences in follicle sensitivity, or simply advanced hair loss that’s less reversible. For these patients, clinicians have historically tried three strategies: switch to oral minoxidil, add finasteride, or increase the topical concentration.
That third option is what drove the emergence of 10%+ formulations — and it’s the one with the most controversy. The FDA has never approved a topical strength above 5% for hair loss, and most mainstream dermatology bodies consider 5% the evidence-based ceiling for routine use.
How Does Minoxidil Work?
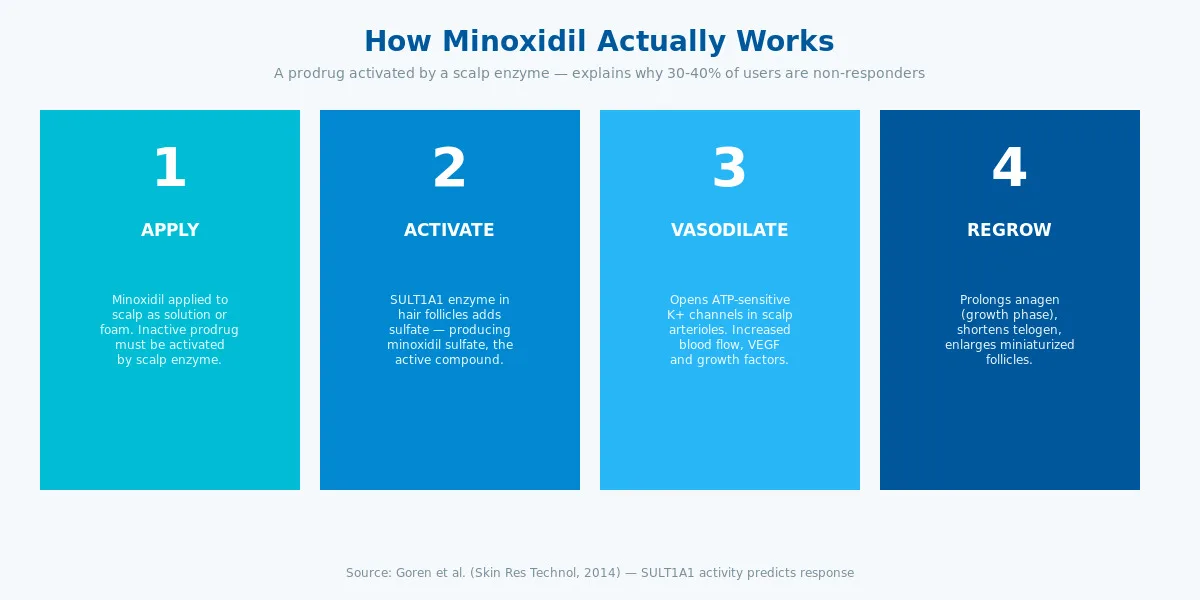
Minoxidil is a prodrug — the molecule applied to the scalp is inactive and must be converted to its active form by an enzyme in hair follicles called sulfotransferase 1A1 (SULT1A1).
Here’s the four-step mechanism:
- Topical absorption. Minoxidil penetrates the stratum corneum and reaches the hair follicle area.
- Sulfation to active drug. SULT1A1 in the outer root sheath of the follicle adds a sulfate group, producing minoxidil sulfate — the actual active compound.
- Potassium channel opening. Minoxidil sulfate opens ATP-sensitive potassium channels on the smooth muscle of scalp arterioles. This causes vasodilation and increases oxygen and nutrient delivery to the follicle.
- Hair cycle modulation. Minoxidil prolongs the anagen (growth) phase of the hair cycle, shortens telogen (rest), and enlarges miniaturised follicles back toward terminal-size thickness. Growth factors including VEGF and prostaglandins are upregulated at the follicle level.
Critically, higher concentrations saturate the scalp’s absorptive capacity and the SULT1A1 enzyme itself. Doubling topical concentration does not double the intra-follicular active drug. This is the main pharmacological reason 10% minoxidil doesn’t deliver twice the hair growth of 5% — there’s a ceiling effect once the enzyme system is saturated.
Key Uses & Applications
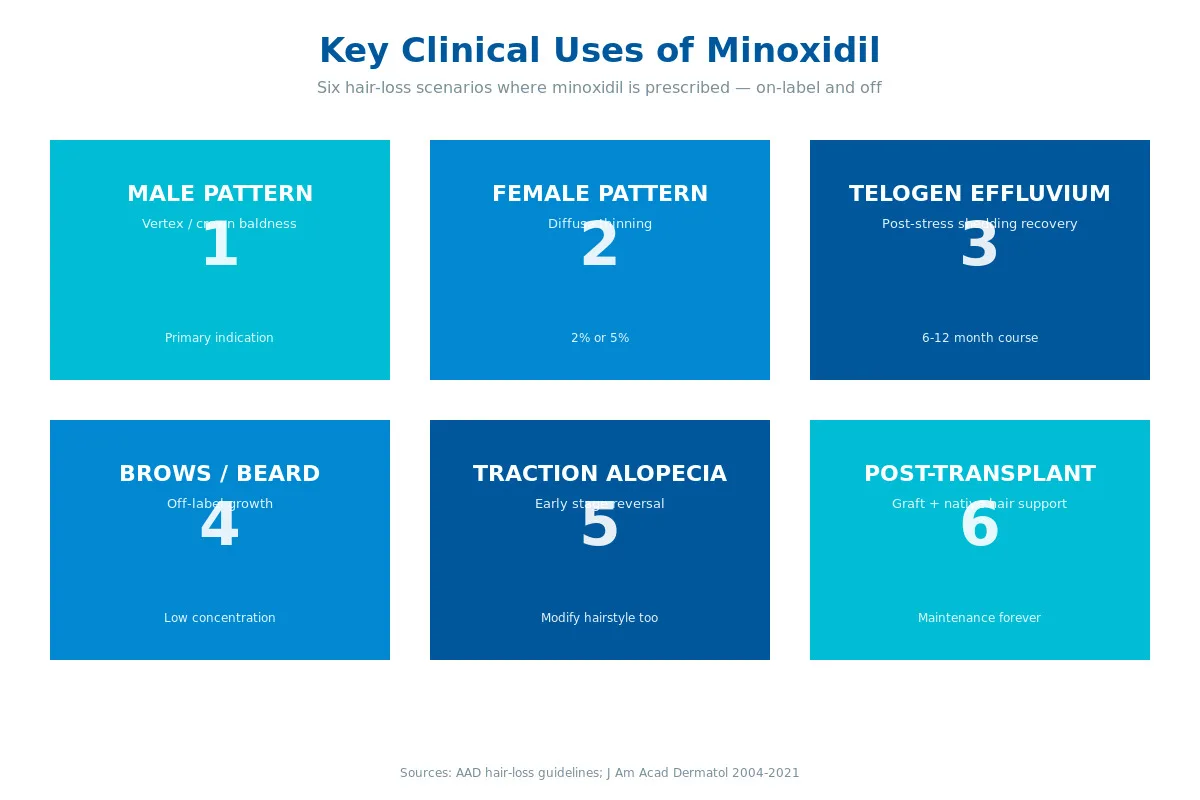
Infographic summary: Male-pattern baldness (vertex/crown) · Female-pattern hair thinning (2% or 5%) · Telogen effluvium recovery · Eyebrow and beard growth (off-label) · Traction alopecia (early stage) · Post-transplant maintenance.
Minoxidil is indicated, on-label or off-label, for a surprising range of hair loss patterns.
Androgenetic Alopecia (Male-Pattern)
The classic indication. Minoxidil is most effective on the vertex (crown) and modestly effective on the frontal hairline — though combination with oral finasteride or dutasteride (see our finasteride vs dutasteride guide) is far superior for frontal recession.
Female-Pattern Hair Loss
2% and 5% topical formulations are both FDA-approved for women. 2% was the original approval; 5% foam followed in 2014. 10% is not recommended for women due to facial hypertrichosis risk.
Telogen Effluvium (Recovery)
Post-partum shedding, stress-induced shedding, and medication-induced shedding all respond to minoxidil 5%. Treatment is typically short — 6 to 12 months — until natural recovery is complete.
Eyebrow and Beard Growth (Off-Label)
Growing use of low-concentration minoxidil for sparse eyebrows or patchy beards, particularly in men under 40.
Traction Alopecia
Helps reverse early traction alopecia when tight hairstyles are also modified. More advanced traction damage is less responsive.
Post-Transplant Maintenance
Many hair transplant surgeons recommend continued 5% minoxidil after transplantation to maintain native hair and support graft survival. Some protocols even start minoxidil 2–4 weeks before the transplant to optimise scalp vascularity, and continue indefinitely afterwards to defend the rest of the hair from continued androgenetic miniaturisation.
Who should NOT use minoxidil
Minoxidil is contraindicated or cautioned in several groups:
- Pregnant or breastfeeding women — pregnancy category C, discontinue before conception if possible.
- Anyone with scalp skin disease (active dermatitis, psoriasis, open wounds) — the irritation risk is amplified and absorption is unpredictable.
- Unexplained sudden hair loss — work up the cause before treating. Acute patchy loss is usually alopecia areata, which needs immunomodulatory therapy, not minoxidil.
- Severe cardiac disease for oral minoxidil — vasodilation can precipitate angina or heart failure in susceptible patients.
- Children under 18 — safety not established; paediatric hair loss needs dermatology evaluation.
If any of these apply, consult a dermatologist or healthcare provider before considering minoxidil — and if it’s still appropriate, they can guide dose and monitoring.
Safety Profile, Side Effects & Dosage
Topical minoxidil has one of the best-characterised safety profiles in dermatology. Millions of users over four decades — most adverse events are mild and reversible.
Common and Rare Side Effects
| Side effect | Typical concentration | Frequency | Severity |
|---|---|---|---|
| Scalp itching / flaking | All | Common (5–15%) | Mild |
| Scalp dryness / burning | All, worse at 10% | Common (5–20%) | Mild |
| Contact dermatitis | More with 10% | Common at high strength | Mild–moderate |
| Hypertrichosis (facial hair) | 5% (women), 10% (any) | Uncommon / common | Cosmetic |
| Initial shedding (“dread shed”) | All | Very common weeks 2–8 | Expected, mild |
| Tachycardia / palpitations | 10%, oral | Rare | Warrants review |
| Lightheadedness / orthostatic symptoms | Oral minoxidil | Uncommon | Mild–moderate |
| Peripheral oedema | Oral minoxidil | Uncommon | Dose-dependent |
| Allergic reaction to propylene glycol | Liquid formulations | Uncommon | Mild |
Key safety notes
- Initial shedding (“dread shed”) is normal and expected. Weeks 2–8 of treatment often show increased shedding as follicles transition from telogen to anagen synchronously. This is actually a sign the drug is working.
- Scalp irritation is concentration-dependent. Moving from 5% to 10% roughly doubles the rate of itch, burning, and contact dermatitis.
- Propylene glycol (used in liquid formulations) is the most common irritant; foam formulations are PG-free.
- Oral minoxidil has cardiovascular effects — monitor heart rate and blood pressure at initiation, especially doses above 2.5 mg/day.
Pregnancy and Breastfeeding
Minoxidil is pregnancy category C. Do not use during pregnancy or breastfeeding. Women planning pregnancy should discontinue treatment.
What about oral minoxidil?
Low-dose oral minoxidil (0.25–5 mg/day) has become a legitimate alternative option in the last five years, particularly for topical non-responders and patients with severe topical irritation. Because it bypasses the scalp SULT1A1 enzyme step entirely, it tends to help patients whose topical form simply isn’t being activated efficiently at the follicle.
Oral minoxidil is off-label for hair loss but backed by large observational studies — notably Vañó-Galván et al. (2021), which tracked 1,404 patients and found effectiveness comparable to topical with manageable side effects. Typical doses are 1.25 mg once daily for men and 0.625–1.25 mg for women, with uptitration based on response and tolerability. Above 2.5 mg/day, clinicians watch more closely for peripheral oedema, tachycardia, and (rarely) orthostatic hypotension. Baseline blood pressure and pulse are reasonable before starting, and any new ankle swelling or palpitations warrant a dose review.
What Does the Research Say?
Minoxidil has been studied in hundreds of clinical trials since the 1980s. Here are the studies most relevant to the 5% vs 10% question.
| Study | Year | Finding | Source |
|---|---|---|---|
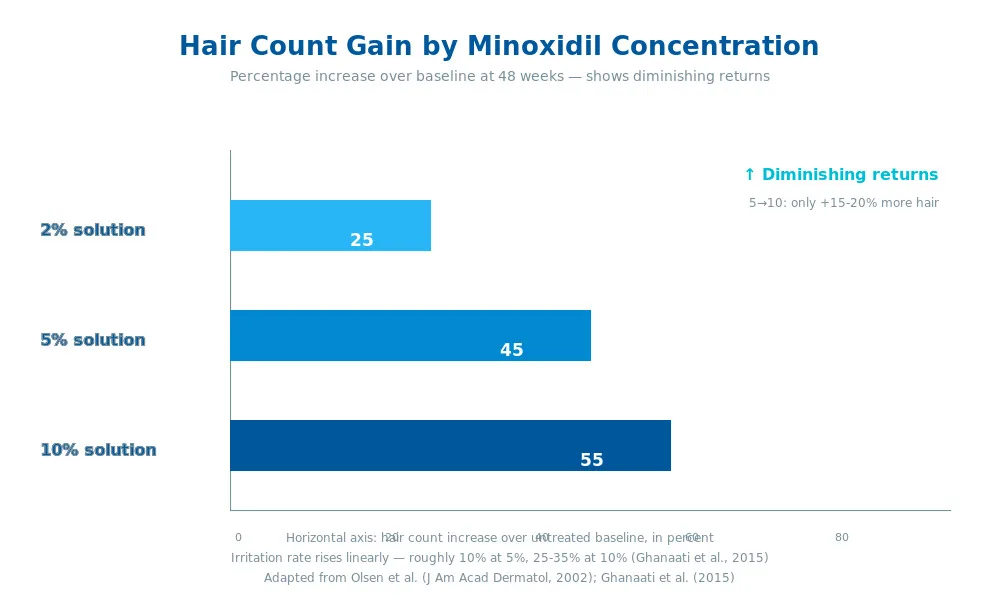
| Olsen et al. | 2002 | 5% minoxidil produced ~45% more hair count at 48 weeks than 2% in men | J Am Acad Dermatol |
| Lucky et al. | 2004 | 5% foam and 2% solution equally effective in women | J Am Acad Dermatol |
| Goren et al. | 2014 | Scalp SULT1A1 activity predicts response — low-activity patients respond poorly at any topical concentration | Skin Res Technol |
| Ghanaati et al. | 2015 | 10% minoxidil had ~15–20% greater hair-count increase vs 5% but with 2.3× more contact dermatitis | J Biomed Mater Res |
| Vañó-Galván et al. | 2021 | Low-dose oral minoxidil (0.25–5 mg) effective for androgenetic alopecia with manageable side effects | J Am Acad Dermatol |
Research suggests the efficacy curve for topical minoxidil flattens markedly above 5%. The step from 2% to 5% produces roughly 40–45% more terminal hair count in male-pattern baldness; the step from 5% to 10% produces only 15–20% more hair count at 48 weeks. Returns diminish while irritation rises approximately in proportion to concentration.
Early studies indicate low-dose oral minoxidil at 1.25–5 mg daily is becoming a preferred alternative for patients who can’t tolerate topical irritation — particularly non-responders to topical 5% who would otherwise escalate to 10%. The oral route bypasses the scalp SULT1A1 enzyme entirely, which may explain why some topical non-responders do well on oral.
See our broader hair-loss coverage at everything you need to know about hair loss, how to stop hair loss, and can you prevent hair loss before it’s too late.
Minoxidil 5% vs 10% — Head-to-Head
| Criterion | Minoxidil 5% | Minoxidil 10% |
|---|---|---|
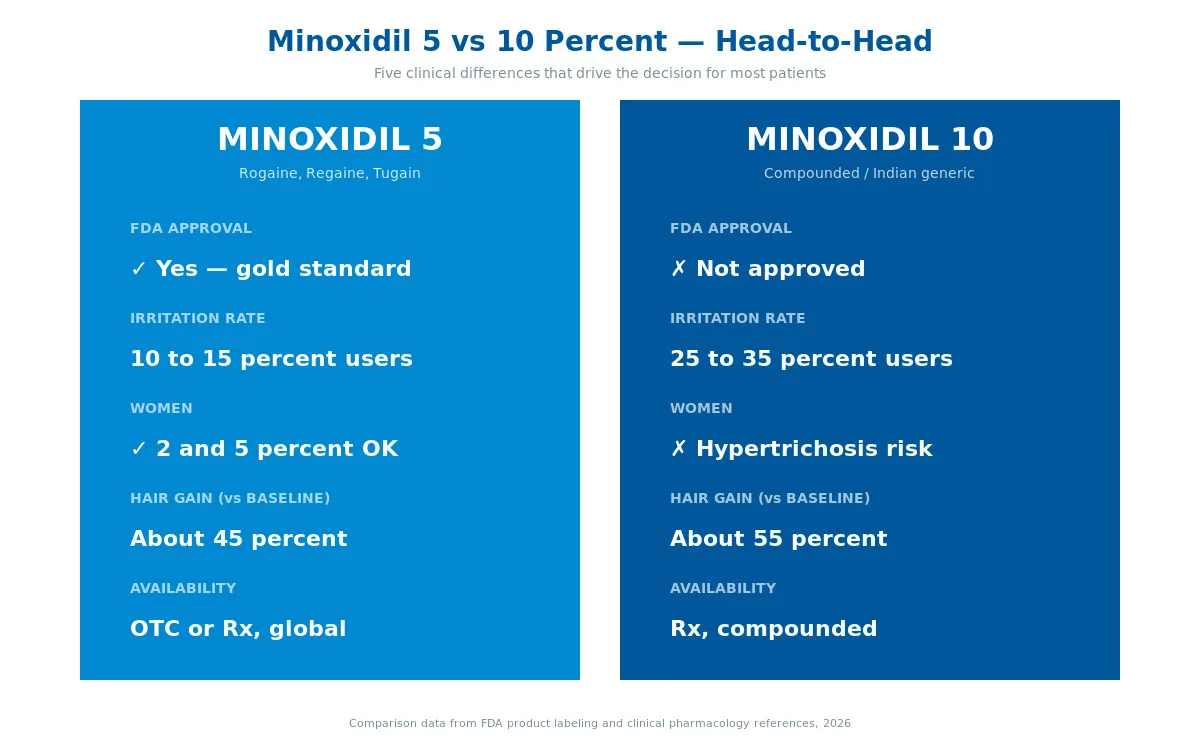
| FDA approval | Yes (men + women) | No (compounded / overseas generic) |
| Typical target user | Most male and female pattern hair loss | Non-responders to 5%, advanced male AGA |
| Formulations | Liquid, foam | Liquid mostly; rare foam |
| Efficacy (hair count at 48 weeks) | ~45% above 2% baseline | ~60% above baseline (+15–20% vs 5%) |
| Scalp irritation rate | ~10–15% | ~25–35% |
| Contact dermatitis | Uncommon | Common |
| Hypertrichosis (facial) risk | Low | Moderate-high — not recommended in women |
| Cardiovascular absorption | Minimal | Slightly increased, still low |
| Daily cost (generic) | Low | Low-moderate |
| Women | Recommended | Not recommended |
| Availability | Pharmacy OTC / Rx | Compounded or international generic |
| Onset of visible results | 3–6 months | 3–6 months |
| Maintenance required | Lifelong | Lifelong |
Bottom line on the head-to-head: 10% minoxidil offers about 15–20% extra hair count vs 5% in studies, but with roughly double the irritation rate. The patients who gain the most from moving to 10% are men who have already fully plateaued on 5% after 12+ months of consistent use. For first-time users or women, 5% is the correct starting point.
How to Use Minoxidil Correctly
Four rules decide whether minoxidil works for you:
- Start with clean, dry scalp. Apply to a towel-dry scalp — not damp, not freshly shampooed without drying. Wet scalp dilutes the drug and reduces follicle uptake.
- 1 mL twice daily. Most solutions come with a dropper marked at 1 mL. Apply to affected areas of the scalp (vertex, crown, or along the part line). Spread gently with fingertips to cover — don’t massage in vigorously.
- Don’t wash or style for 4 hours. Minoxidil needs time to absorb. Most guidance suggests letting it dry fully (usually 20–30 minutes) before styling products, hats, or pillow contact.
- Be patient — minimum 3 to 6 months. Visible regrowth is slow. The first 8 weeks often include “dread shed.” Don’t judge efficacy before 6 months of continuous use.
Practical tips
- Wash hands thoroughly after application to avoid transferring the drug to the face (causes facial hair) or eyes (causes irritation).
- Apply at consistent times — morning and bedtime are typical.
- If switching from 5% to 10%, expect an adjustment period of 2–4 weeks with increased scalp tightness or flaking.
- Foam formulations (Tugain Foam, Rogaine Foam) are PG-free and suit irritation-prone users.
- Don’t double up missed doses — just resume at the next scheduled time.
- Oral low-dose minoxidil (0.625–2.5 mg daily) is a clinician-supervised alternative for topical non-responders.
Browse our full minoxidil range — Tugain Foam, Tugain Solution, Regaine 5%, Mintop Lotion, Minoxytop (Minoxidil), Lonitab — all shipped discreetly worldwide.
Frequently Asked Questions
Is 10% minoxidil better than 5%?
In clinical trials, 10% produces about 15–20% greater hair-count increase than 5% at 48 weeks — a measurable but modest gain. The trade-off is significantly more scalp irritation, roughly doubling the rate of itching, burning, and contact dermatitis. For most users starting treatment, 5% is the right place to begin. Moving to 10% makes most sense for men who have plateaued on 5% after at least 12 months of consistent use.
Can I switch from 5% to 10% minoxidil?
Yes, but only after you’ve given 5% a full fair trial — at least 12 months of consistent twice-daily use with good compliance. Switching earlier doesn’t give 5% enough time to show its full effect (most gains happen between months 6 and 12). When you switch, expect a 2–4 week adjustment period with increased scalp tightness. If irritation becomes significant, drop back to 5% or consider oral low-dose minoxidil.
Is 10% minoxidil safe for women?
Generally no. The main concern is facial hypertrichosis — unwanted hair growth on the forehead, cheeks, and upper lip from systemic absorption or transfer via hands. This is uncommon at 5% in women but becomes common at 10%. Most dermatologists advise women to stay at 2% or 5% and explore oral minoxidil if topical isn’t working, rather than escalating to 10%.
How long does 10% minoxidil take to work?
The same as 5% — minimum 3 months for early signs, 6 months for reliable visible results, and 12 months for full effect. The higher concentration does not speed up the hair cycle; it just delivers more active drug per dose, which increases the absolute amount of regrowth but not the timeline. Expect the same “dread shed” at weeks 2–8.
What’s the strongest minoxidil available?
Commercially available concentrations go up to 15% (mainly Indian compounded products) and very occasionally 20% in specialty formulations. Beyond 10%, the diminishing-returns curve becomes very steep — you get minimal extra hair growth while irritation rises sharply. Most hair-loss specialists consider 10% the practical ceiling for topical therapy; above that, switching to oral minoxidil makes more sense.
Does minoxidil work better with finasteride?
Yes — combination therapy is the most effective medical approach for male-pattern baldness. Minoxidil stimulates growth; finasteride blocks the hormonal cause. Multiple studies show combination therapy produces better outcomes than either drug alone — often cited as a roughly 10–15% boost over monotherapy. See our finasteride vs dutasteride comparison for the DHT-blocker side of the equation.
Do I lose the gains if I stop minoxidil?
Yes, within 3–6 months. Minoxidil doesn’t “cure” hair loss — it maintains and reverses it while being applied. Stopping treatment allows the underlying genetic process to resume, and regrown hair is typically shed within 90–180 days of discontinuation. This is why minoxidil treatment is considered lifelong for ongoing pattern hair loss.
Is oral minoxidil better than 10% topical?
For non-responders or patients with severe topical irritation, yes, often. Low-dose oral minoxidil (0.625–5 mg/day) bypasses the SULT1A1 enzyme entirely, so it helps patients whose scalps don’t activate the topical form well. It’s off-label but has strong evidence (Vañó-Galván et al., 2021). The trade-off: it requires prescriber monitoring for blood pressure, heart rate, and peripheral oedema, especially at doses above 2.5 mg/day.
The Bottom Line
The minoxidil 5% vs 10% debate mostly resolves to a single principle: higher concentration delivers modestly better regrowth at the cost of considerably more scalp irritation. For first-time users, 5% is the evidence-based starting point and the FDA-approved standard. For men who have stuck with 5% for 12+ months and plateaued, 10% is a reasonable next step under a dermatologist’s supervision.
For women, stay at 2% or 5% — the facial hair risk from 10% usually isn’t worth the small efficacy bump. For anyone with significant scalp irritation on 5%, oral low-dose minoxidil is probably a better next step than escalating topical concentration.
Decision summary — how most dermatologists actually choose
- First-time male user, moderate vertex thinning: minoxidil 5% twice daily + consider adding finasteride 1 mg.
- First-time female user, diffuse thinning: minoxidil 5% foam once daily (or 2% liquid BID).
- Male plateau after 12+ months on 5%: consider 10% (or switch to low-dose oral minoxidil).
- Woman plateau on 5%: switch to low-dose oral minoxidil — not to 10%.
- Significant scalp irritation on 5%: switch to 5% foam first, then to oral if foam still irritates.
- Post-hair-transplant: 5% solution or foam indefinitely for maintenance.
Whichever route you choose, the three rules are the same: apply consistently, give it at least 6 months, and combine with finasteride or dutasteride if you want maximum male-pattern coverage.
Ready to explore your options? Browse our minoxidil catalogue or speak to your healthcare provider about which concentration fits your hair-loss pattern.
Last medical review: April 2026. Next scheduled review: October 2026.
Authoritative references: AAD pattern hair loss · NHS androgenetic alopecia · Olsen EA et al. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol 2002;47:377-385. · Vañó-Galván S et al. Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. J Am Acad Dermatol 2021;84:1644-1651.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.