







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Most dry eye advice hands you a bottle of artificial tears and tells you to keep dripping. That advice treats dry eye as a flat, constant problem. It isn’t. For most people it simmers at a manageable baseline and then spikes — a week of wind, a deadline spent staring at a screen, a flight, a season change.
Eysuvis eye drops exist for those spikes. They were the first corticosteroid approved specifically for the short-term treatment of dry eye flares, and that “short-term” is not marketing softness — it is printed on the label as a hard two-week ceiling. This guide covers what the drops do, the clever delivery trick behind them, what the pooled trial data actually showed, the two-week rule and why it exists, and which drops do a similar job.
There is one number in the safety data that explains the whole design of this drug. We will get to it.
Key takeaways
- Eysuvis is loteprednol etabonate 0.25% — a lower strength than other loteprednol drops, and that is deliberate.
- It treats flares, not the baseline. Using it as a daily maintenance drop misunderstands the drug entirely.
- The label caps it at two weeks — there is a specific reason, covered in the safety section.
- It is a “soft” steroid, engineered to fall apart after it works — and one number in the trial data shows why that matters.
- A delivery trick gets several times more drug past your tear film than ordinary drops manage.
- Steroids and cyclosporine are not rivals — they do opposite jobs, and many people need both.
What Are Eysuvis Eye Drops? (Definition & Background)
Eysuvis eye drops are an ophthalmic suspension of loteprednol etabonate 0.25%, a topical corticosteroid. Their approved use is the short-term treatment of the signs and symptoms of dry eye disease, for up to two weeks at a time. They calm inflammation on the eye’s surface rather than lubricating it.
That approval matters more than it sounds. Dry eye had plenty of long-term treatments — lubricants, cyclosporine, lifitegrast — but no steroid formally approved for the flares that punctuate the condition. Eye doctors had long prescribed steroids off-label for exactly this, using drops designed for post-surgical inflammation. Eysuvis was the first product developed and approved for the flare itself.
The strength that confuses people
Here is the counterintuitive part. Loteprednol also comes as a 0.5% drop — twice the concentration — sold under names like Lotemax for post-operative inflammation and other inflammatory eye conditions. Eysuvis is the weaker 0.25%.
People reasonably assume weaker means less effective. It doesn’t, because concentration is only half the equation. The other half is how much of that drug actually gets where it needs to go, which is the subject of the next section. A smarter delivery system means you need less steroid on the eye — and with steroids, less is genuinely better.
What it is not
- Not a lubricant. It does not replace artificial tears; it treats the inflammation underneath.
- Not a maintenance drop. The two-week limit is structural, not a suggestion.
- Not an antibiotic. It treats inflammation, not infection — and can make some eye infections worse.
- Not the same as cyclosporine. Different drug class, different timeline, different job.
How Do Eysuvis Eye Drops Work? (The Science, Simply)
Loteprednol is a corticosteroid: it switches off the inflammatory signalling that makes a dry eye surface red, sore and gritty. What makes Eysuvis different is not the steroid but the delivery — particles engineered to slip through the eye’s mucus barrier instead of being trapped by it.
Your tear film is not just salty water. It carries a sticky mucus layer whose job is to catch foreign particles and sweep them away. It cannot tell the difference between grit and medicine, so it traps most of an ordinary eye drop and blinks it into your tear duct within minutes.
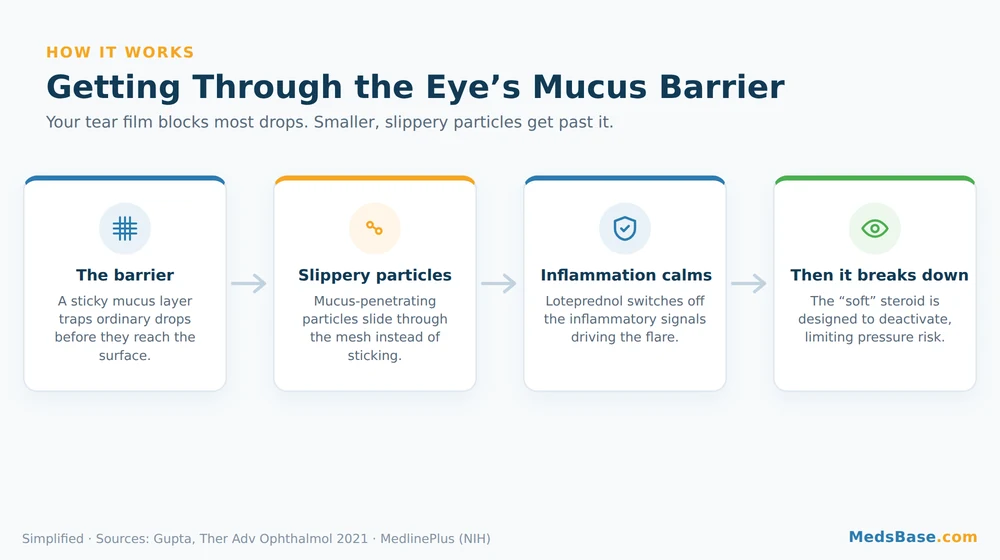
Think of the mucus layer as a fine net over a doorway. Ordinary drug particles are sticky and lumpy, so they snag on the net. Mucus-penetrating particles are made smaller and given a slippery coating, so they pass through the mesh and reach the tissue behind it. Same drug, better door.
The “soft steroid” design
This is the part that makes repeated short courses defensible, and it comes down to chemistry.
Traditional eye steroids like prednisolone and dexamethasone are ketone-based. They are effective, but they hang around, and lingering steroid on the eye is what drives the classic complications — raised pressure inside the eye, cataract, slowed healing.
Loteprednol is an ester-based steroid, sometimes called a “soft” or “retrometabolic” steroid. It is designed to do its anti-inflammatory work and then be broken down by the eye’s own enzymes into inactive by-products. It is built with an off-switch. Whether that translates into a real-world safety advantage is a question the research section answers with an actual number.
Why Dry Eye Flares Change the Treatment
A dry eye flare is a temporary worsening of symptoms above your usual baseline, often triggered by screens, wind, air conditioning, allergens, travel or contact lens wear. Flares are inflammatory surges — which is why lubricating drops soothe them but rarely stop them.
This is the framing that most dry eye content misses entirely, and it changes what “treatment” even means.

Take Priya, 44, an illustrative example of a very common pattern. She has mild dry eye that artificial tears handle fine most of the year. Then comes a month of deadlines: ten-hour screen days, air conditioning, four hours of sleep. Her eyes go from mildly gritty to burning and red. She doubles her artificial tears and gets twenty minutes of relief at a time, because tears are washing a fire, not putting it out.
What Priya has is not worse baseline dry eye. It is a flare — an inflammatory surge sitting on top of her baseline. Two different problems, two different tools:
- The baseline needs maintenance: lubricants, lid hygiene, omega-3s, and for some people cyclosporine or lifitegrast. These work slowly and continuously.
- The flare needs something that works in days and then gets out. That is what a short steroid course is for.
Here is why this distinction has teeth. Maintenance drugs are famously slow — cyclosporine can take months to show its full benefit, and it can sting at first. Someone in the middle of a flare who starts cyclosporine and expects relief next week concludes it “doesn’t work” and quits before it ever had a chance. Eye-care professionals see that pattern constantly. Increasingly the approach is to use a steroid to break the flare while the maintenance therapy builds up underneath — treating the wave and the water level as separate jobs.
Who is this for? Who should avoid it?
Likely a good fit: people with diagnosed dry eye disease who get periodic flares that lubricants alone don’t settle; people starting a slow maintenance therapy who need bridging relief; people with a predictable trigger (a heavy travel month, a seasonal spike) under professional guidance.
Should avoid or use extra caution: anyone with an active eye infection — steroids can worsen viral, fungal and bacterial eye infections. Anyone with glaucoma or a history of steroid-related eye-pressure rises needs monitoring and may need a different option. Not for people who have had a recent eye injury or who are healing from eye surgery without specific direction. Contact lens wearers need to check timing, because the preservative can be absorbed by soft lenses.
Always individual: if your “dry eye” has never actually been examined by an eye-care professional, that is the step to take before any steroid. Several conditions mimic dry eye and a few of them get worse on steroids.
Eysuvis Eye Drops Side Effects, Dosage & the Two-Week Rule
The usual dose is one to two drops into each eye four times daily, for a maximum of two weeks. The most common complaint is brief stinging on instillation. The two-week ceiling exists because the risks of topical steroids — raised eye pressure, cataract, delayed healing, masked infection — are driven by duration of use.
Let’s be straight about what a steroid on the eye can do, without either hiding it or catastrophising it.
| Side effect | Frequency | Severity | What to do |
|---|---|---|---|
| Stinging or pain when the drop goes in | Most common (about 5% in trials) | Mild, brief | Usually settles. Refrigerating the bottle can help some people. |
| Blurred vision just after use | Common | Mild, temporary | It is a suspension — wait a minute before driving or reading. |
| Raised pressure inside the eye | Uncommon (0.6% vs 0.2% on placebo in pooled trials) | Potentially serious if missed | Why courses beyond two weeks need a pressure check first. |
| Worsening of an existing eye infection | Uncommon | Serious | Never start a steroid in an undiagnosed red, painful eye. |
| Delayed healing of the eye surface | Uncommon | Moderate | Matters most after injury or surgery — tell your professional. |
| Cataract formation | Rare with short courses; a prolonged-use risk | Serious but treatable | The main reason the label caps duration. |
Why two weeks, specifically?
This resolves the loop from the intro, and the number is the point.
Steroid eye complications are overwhelmingly a function of how long the drug sits on the eye, not how strong a single drop is. Manufacturer labelling for Eysuvis is explicit: treatment is for up to two weeks, and renewing beyond that calls for an examination with magnification and a check of eye pressure. It is one of the few eye drops whose approved use has an expiry date built into the instructions.
That is not a warning about this particular drug being dangerous. It is the opposite — it is the design working. The whole product is built around the idea of a short, intense, self-limiting course. Stretching it into a maintenance drop takes a medicine engineered for two weeks and uses it in the exact way its safety data does not cover.
When to contact your eye-care professional
- Eye pain that gets worse rather than better
- Any change in vision that does not clear within a minute or two of a drop
- Increasing redness, discharge, or light sensitivity
- Symptoms that have not improved by the end of a two-week course — that is information, not a reason to continue
- Seeing halos around lights, which can signal a pressure problem
What Does the Research Say?
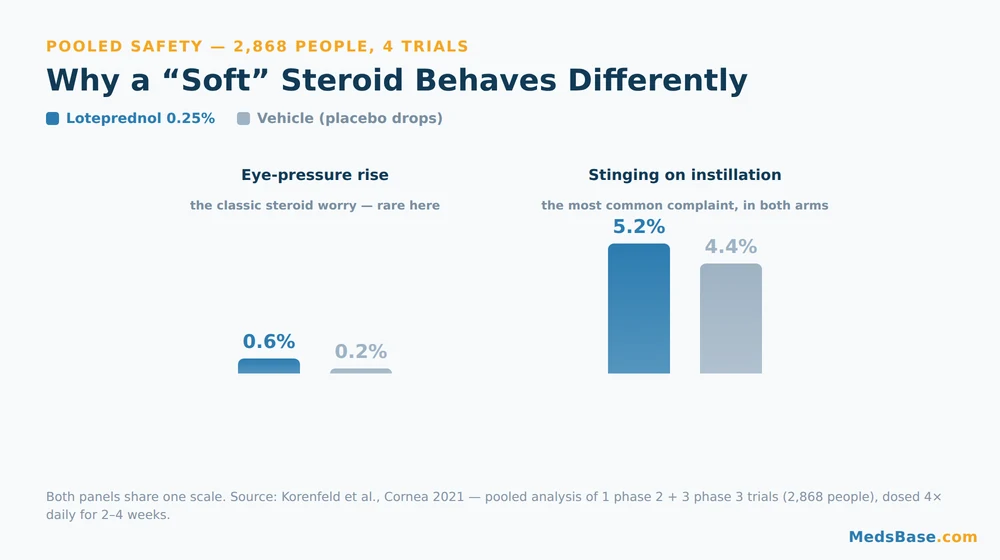
The evidence base is unusually large for a dry eye drug: four randomised, vehicle-controlled trials — one phase 2 and three phase 3 — enrolling roughly 2,900 people between them. The efficacy findings are modest and honest; the safety findings are where the design proves itself.
| Study | Year | What it found | Source |
|---|---|---|---|
| Pooled safety analysis (Korenfeld et al.) | 2021 | Across 4 trials and 2,868 people, eye-pressure elevation occurred in 0.6% on loteprednol 0.25% vs 0.2% on vehicle. Instillation-site pain was the most common event (5.2% vs 4.4%). Judged safe and well tolerated dosed 4× daily for 2–4 weeks. | Cornea |
| Mechanism review (Gupta et al.) | 2021 | Dry eye “often presents with periodic flares” that long-term treatments were not designed for. Mucus-penetrating particles achieved 3.6× greater corneal penetration of loteprednol than conventional suspensions in animal models. | Ther Adv Ophthalmol |
| Manufacturer labelling (clinical studies) | Current | In 4 controlled trials of ~2,900 people over 2 weeks, “a larger reduction in ocular discomfort severity favoring EYSUVIS was observed at Day 15”, and a larger reduction in redness at Day 15 in all four trials. | DailyMed (NIH) |
What this means for you: the eye-pressure signal — the thing that makes clinicians cautious about steroids on the eye — came out at 0.6% versus 0.2% on placebo drops. Small, and close to the placebo rate. That is the number that justifies the whole “soft steroid” concept, and it is why this drug can be considered for repeated short courses when older steroids could not.
Now the honest caveats, because they matter. The efficacy is real but not dramatic: the trials measured improvements in discomfort and redness over two weeks, and the labelling describes them qualitatively rather than as a headline percentage. Not every endpoint hit significance in every trial. The 3.6-fold penetration figure comes from animal models, not human eyes. And a low pressure-rise rate over two to four weeks tells you nothing about what repeated courses year after year would do — that study has not been done. This is a useful tool with a genuine evidence base, not a breakthrough.
Eysuvis vs Other Dry Eye Treatments
The most common mistake here is treating these options as competitors. They are not. They do different jobs on different timescales, and the right answer for most people involves more than one.
| Option | Job it does | How fast | How long you use it | Main drawback |
|---|---|---|---|---|
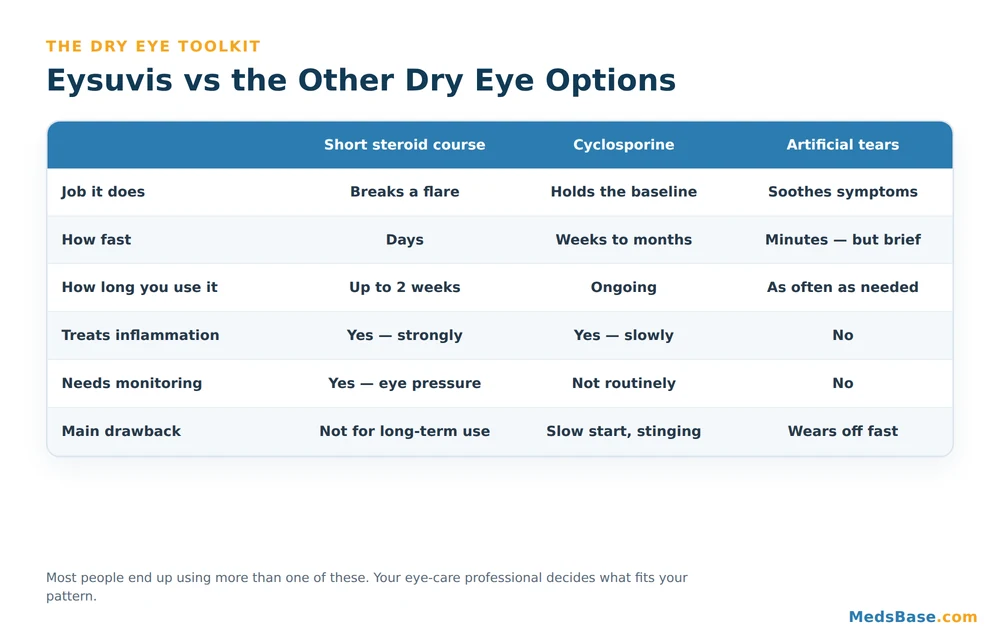
| Loteprednol 0.25% (Eysuvis) | Breaks a flare | Days | Up to 2 weeks | Not for long-term use; needs pressure checks if repeated |
| Loteprednol 0.5% | Stronger inflammation control (post-op, uveitis, allergy) | Days | Short courses | Formulated for other conditions, not dry eye flares |
| Cyclosporine 0.05% | Holds the baseline; helps eyes make more tears | Weeks to months | Ongoing | Slow to start; stinging early on |
| Artificial tears | Soothes and lubricates | Minutes | As often as needed | Wears off fast; no effect on inflammation |
| Fluorometholone | Lower-potency steroid alternative | Days | Short courses | Also needs pressure monitoring |
Which fits which situation? If your eyes are flaring right now and tears aren’t touching it, the flare is inflammatory and a short steroid course is the category that addresses it. We stock the same molecule as Lotepred loteprednol eye drops, though at the 0.5% strength used for inflammatory eye conditions rather than the 0.25% dry-eye formulation — which strength suits you is a decision for your eye-care professional, not a shopping choice. If your problem is a grinding daily baseline rather than episodic spikes, maintenance therapy is the better target: Restasis cyclosporine drops are the long-game option. And if you simply need relief between the two, preservative-conscious lubricating artificial tears remain the everyday workhorse.
A note on availability, because it is a fair question: the specific Eysuvis-branded 0.25% product is not something we stock, and this guide is not an attempt to sell you a substitute for it. The useful thing to take away is the category — if you and your professional decide a short steroid course is right, loteprednol is the molecule you are discussing.
How to Use Eysuvis Eye Drops — Practical Guidance
Getting the technique right matters more with this drop than with most, for one specific reason: it is a suspension, not a solution. The medicine is suspended in liquid and settles when the bottle sits still.
- Wash your hands, then shake the bottle well. An unshaken suspension gives you an uneven dose — watery early in the bottle, over-concentrated later.
- Tilt your head back and pull the lower lid down to make a small pocket.
- Drop one to two drops into the pocket — not directly onto the eyeball, which triggers a reflex blink that ejects most of it.
- Close your eye gently for about a minute. Don’t squeeze or blink hard; that pumps the drop into your tear duct.
- Press lightly at the inner corner of your eye for 30 seconds if you want to keep more of the drug on the eye.
- Repeat four times daily, and stop at two weeks unless your professional has examined you and said otherwise.
Mistakes to avoid
- Not shaking the bottle. The single most common technique error with any suspension drop.
- Letting the tip touch your eye or lashes. That contaminates the bottle — a real problem with a drug that suppresses local immunity.
- Stacking drops back to back. Your eye holds one drop’s volume. If you use other drops, space them at least five minutes apart.
- Leaving soft contact lenses in. The preservative can be absorbed by the lens; take them out and wait about 15 minutes before putting them back.
- Quietly extending the course. Two weeks means two weeks unless you have been re-examined.
- Treating an undiagnosed red eye. If nobody has looked at your eye with a slit lamp, a steroid is a gamble.
Related reading
- Xalatan (latanoprost) eye drops guide — useful if eye pressure is the thing you have been told to watch.
- Best glaucoma eye drops compared — what actually lowers pressure, if a steroid pushed yours up.
- Combigan (brimonidine/timolol) guide — a combination option in the same pressure-lowering family.
Frequently Asked Questions
Q: What are Eysuvis eye drops used for?
A: Eysuvis eye drops are used for the short-term treatment of the signs and symptoms of dry eye disease — specifically for flares, when symptoms surge above their usual level. They are a corticosteroid that reduces inflammation on the eye’s surface, dosed four times daily for up to two weeks. They are not a lubricant and not a daily maintenance treatment, so most people use them alongside other dry eye measures rather than instead of them.
Q: How long does it take Eysuvis to work?
A: Most improvement in the trials was assessed over a two-week course, with results measured at around Day 15. Many people notice their symptoms easing within the first several days, but the drops are designed to be judged across the full course rather than in the first 48 hours. If two weeks pass with no improvement, that is meaningful information for your eye-care professional — not a reason to keep going on your own.
Q: Why can you only use Eysuvis for two weeks?
A: Because the risks of topical steroids — raised eye pressure, cataract, delayed healing and masked infection — are driven mainly by how long the drug is used, not by a single dose. The labelling caps treatment at two weeks and says that renewal beyond that requires an examination with magnification and a check of eye pressure. The two-week limit is a designed safety feature of a short-course drug, not a hint that it is unusually dangerous.
Q: Is Eysuvis a steroid, and is that safe for eyes?
A: Yes, it is a corticosteroid — loteprednol etabonate. It belongs to the “soft” steroid group: ester-based molecules designed to break down into inactive by-products after they act, unlike older ketone steroids that linger. In a pooled analysis of four trials in 2,868 people, eye-pressure elevation occurred in 0.6% on loteprednol versus 0.2% on placebo drops. Short courses under supervision are generally well tolerated; prolonged unsupervised use is where steroids cause trouble.
Q: What is the difference between Eysuvis and Lotemax?
A: Both are loteprednol etabonate, but at different strengths and for different jobs. Eysuvis is 0.25% and approved for short-term dry eye flares, using a mucus-penetrating particle formulation that delivers more drug to the eye surface. Lotemax is 0.5% and used for other inflammatory eye conditions, including after eye surgery. The lower Eysuvis concentration is deliberate: better delivery means less steroid is needed on the eye.
Q: Can I use Eysuvis and artificial tears together?
A: Generally yes, and many people do — they do completely different jobs. The steroid treats the inflammation driving a flare; the tears lubricate and soothe. The practical rule is spacing: leave at least five minutes between different eye drops, because your eye can only hold about one drop’s worth of liquid at a time. Putting them in back to back mostly just washes the first one out. Confirm your specific combination with your eye-care professional.
Q: Is Eysuvis the same as Restasis?
A: No — different drug class and, more importantly, a different purpose. Restasis is cyclosporine, an immune-modulating drop taken long-term to help your eyes produce more of their own tears; it can take weeks to months to reach full effect. Eysuvis is a steroid for short bursts of inflammation. They are frequently used together rather than as alternatives, with the steroid breaking a flare while the cyclosporine slowly builds the baseline underneath.
Q: Can I wear contact lenses with Eysuvis?
A: Not while you put the drops in. Loteprednol drops contain benzalkonium chloride, a preservative that soft contact lenses can absorb. The standard guidance is to remove your lenses before instilling the drop and wait about 15 minutes before putting them back in. Since contact lens wear is itself a common dry eye flare trigger, it is worth asking your eye-care professional whether a break from lenses would help during the course.
The Bottom Line on Eysuvis Eye Drops
Eysuvis eye drops are a narrow tool used well: a soft steroid, at a low concentration, delivered cleverly, for a specific two-week job. The evidence behind them is solid rather than spectacular — modest improvements in discomfort and redness, with a reassuringly low eye-pressure signal that justifies the whole design. What they are genuinely good at is the thing artificial tears cannot do: pulling a flare back down quickly.
The bigger idea outlasts the brand. If you take one thing from this guide, make it this: dry eye is a condition with a baseline and waves, and treating only one of them is why so many people feel stuck. Most people need something for the water level and something else for the wave.
One thing to do this week: spend two minutes working out which problem you actually have. If your eyes are consistently gritty every day, that is a baseline problem and maintenance therapy is your conversation. If they are fine for weeks and then miserable for ten days at a stretch, you have flares — and that is a specific thing to say out loud at your next appointment, because it changes what gets recommended. Either way, get the eye examined before any steroid goes into it.
Still working out your next step?
- Been told to keep an eye on your eye pressure? Our guide to the drops that lower it explains the options.
- Want the wider picture on prescription eye drops and what each class does? Start with the eye care range.
Sources and further reading
- Loteprednol ophthalmic — MedlinePlus (US National Library of Medicine)
- EYSUVIS (loteprednol etabonate 0.25%) labelling — DailyMed, NIH
- Dry Eye — National Eye Institute (NIH)
- Dry eyes — NHS
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.