







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
💡 Quick Answer
Duphaston is the brand name for dydrogesterone 10 mg, a tablet that mimics progesterone. It is used for irregular or absent periods, heavy bleeding, endometriosis, PMS, and to protect the womb lining during HRT. Despite being a hormone, it is not a contraceptive and will not prevent pregnancy.
Here is the fact that surprises almost everyone handed this tablet: Duphaston is a hormone that behaves like progesterone, yet will not stop you getting pregnant. Many assume any progestogen works like the mini-pill. It does not, and that assumption is how unplanned pregnancies happen.
In the United States you hit a second puzzle: you cannot buy Duphaston there at all. That absence reads as a red flag — surely it was banned for a reason? The paperwork says otherwise, and we will get to exactly what the FDA put in writing.
By the end you will know what dydrogesterone does, which cycle days you take it on and why that matters more than the dose, what the trials found, and where the honest limits of the evidence sit.

Key Takeaways
- It is a progestogen, not birth control — and the label says so in plain terms.
- Its mirrored structure is the whole story: it explains why it works as a tablet and why acne and hair growth are rarely a problem.
- The cycle days matter more than the dose — one counting error makes a course look useless.
- In IVF, an oral tablet matched a vaginal gel across 1,000+ women — with a caveat about what “matched” means.
- The FDA stated in writing that it was not withdrawn from the US for safety or effectiveness reasons.
- One 2015 study raised a heart-defect worry. A larger 2024 review looked again — we cover both.
What Is Duphaston?
Duphaston is the brand name for dydrogesterone, a laboratory-made hormone that closely mimics progesterone — the hormone your ovaries produce in the second half of every cycle. Each tablet contains 10 mg. Doctors reach for it when your own progesterone is too low, or when an estrogen needs balancing.
The drug is not new. Dydrogesterone has treated progesterone-related conditions since the 1960s — six decades of real-world use across a hundred-plus countries. That longevity counts in a field where newer often means thinner evidence.
Progesterone has one job in the cycle: it takes a womb lining that estrogen has thickened and switches it into a stable, “secretory” state — ready either to support a pregnancy or to shed cleanly. When your body does not make enough, that switch never flips. Periods turn erratic, bleeding gets heavy, and the lining keeps building instead of resetting.
Duphaston steps in and flips that switch. That single mechanism explains almost every use on its label, which is why one tablet can appear to treat conditions as different as PMS and menopause care. They are the same underlying shortfall wearing different clothes.
One clarification, because it trips people up constantly: progesterone and progestogen are not synonyms. Progesterone is the hormone your body makes. “Progestogen” is the family name for anything acting on the progesterone receptor — including dydrogesterone, norethisterone, and the hormones in contraceptive pills. Family members behave very differently. Assuming otherwise is the root of most confusion about Duphaston.
How Does Dydrogesterone Work?
Dydrogesterone is a retroprogesterone: a near-mirror of progesterone in which part of the steroid skeleton is flipped, giving a bent, rigid molecule rather than a flat one. That structural quirk is not trivia — it is the reason the drug behaves the way it does in your body.
Think of steroid hormones as keys, and receptors as locks. Progesterone is a slightly floppy key that fits its own lock well but also rattles around in a few neighbouring ones. Dydrogesterone’s bend makes it a stiffer, more precisely cut key. It turns the progesterone lock firmly, and barely engages the others at all.
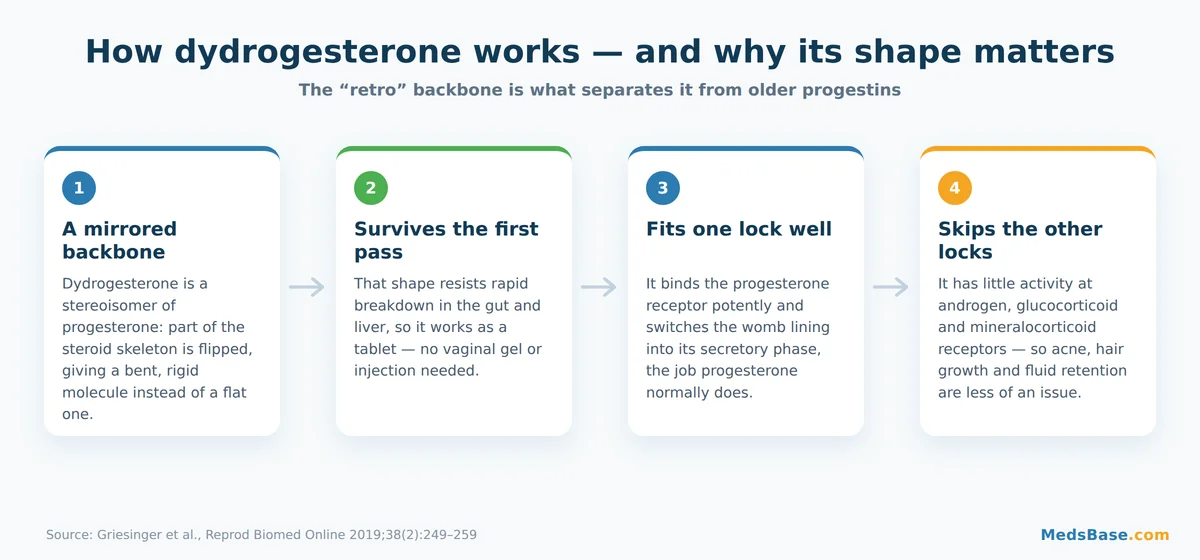
Two consequences follow, and both matter to you directly.
First, Duphaston survives being swallowed. Plain progesterone is broken down so fast by the gut and liver that oral dosing is inefficient — which is why micronised progesterone is so often prescribed as a vaginal capsule or gel. Dydrogesterone has high oral bioavailability. In practice, that is the difference between a tablet with breakfast and a vaginal gel you schedule your day around.
Second, it skips the receptors that cause grief. Older progestogens derived from testosterone can nudge androgen receptors, producing acne, oily skin and unwanted hair growth. Dydrogesterone has little activity at androgen, glucocorticoid or mineralocorticoid receptors. Fewer side doors opened means fewer side effects.
🔬 Research Spotlight
A 2019 pharmacological review in Reproductive BioMedicine Online by Griesinger and colleagues examined why dydrogesterone behaves differently from other progestogens. Its conclusion is the practical one: this is a stereoisomer of progesterone with high oral bioavailability, used since the 1960s, and more recently approved for luteal phase support in assisted reproduction. Read the review on PubMed.
Here is where it gets interesting. That same selectivity has a flip side most articles skip — and it is the most important thing on this page.
Duphaston Uses — What It Actually Treats
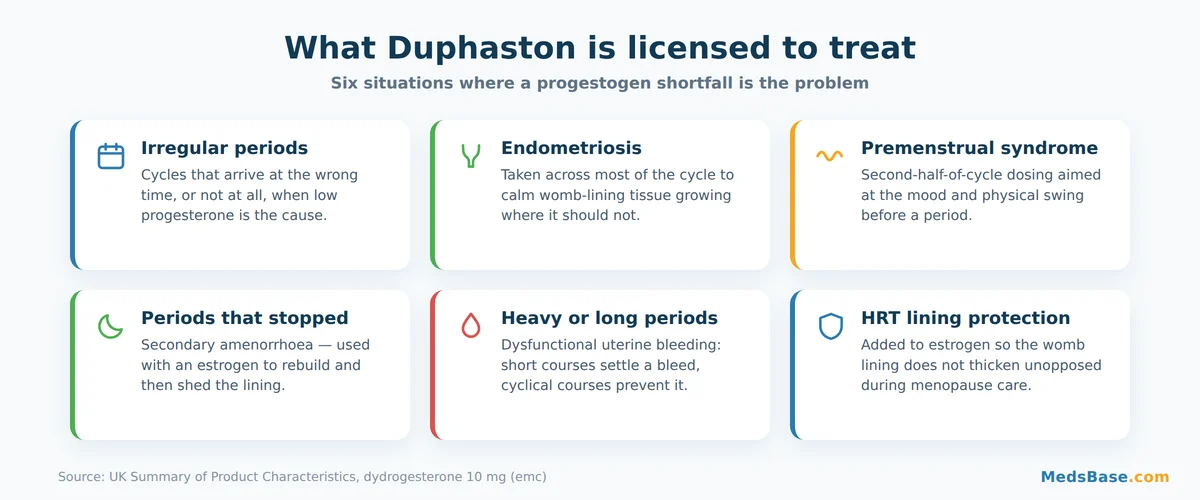
Duphaston uses cluster around one theme: your own progesterone is not doing its job, or an estrogen needs a counterweight. The UK licence covers six scenarios, each with its own cycle-day schedule.
✅ Who Is This For? / Who Should Avoid It?
It may suit you if: your periods are irregular, absent, heavy or prolonged and low progesterone is the suspected cause; you have endometriosis or PMS; or you take estrogen for menopause and still have your womb.
It is not for you if: you want contraception; you have uninvestigated vaginal bleeding; a progestogen-sensitive tumour; serious liver disease or a history of liver tumours; a thromboembolic disorder; or an allergy to any ingredient. Unexplained bleeding needs a diagnosis first — treating the symptom can mask the cause.
Duphaston for irregular periods and cycles that stopped
If you ovulate erratically, you produce progesterone erratically, and your cycle loses its rhythm. Duphaston for irregular periods works by supplying the missing signal across the second half of the cycle: the lining matures on schedule, then sheds when the tablets stop. That withdrawal bleed is the point, not a side effect.
For secondary amenorrhoea — periods stopped for reasons other than pregnancy or menopause — Duphaston is usually paired with an estrogen. The estrogen rebuilds a lining worth shedding; the dydrogesterone tells it when to go.
Heavy or prolonged bleeding
Dysfunctional uterine bleeding often reflects a lining thickened by estrogen with no progesterone to stabilise it. Two approaches: a short course to settle a bleed now, or a cyclical course to stop it recurring. Different schedules, different goals — and mixing them up is common.
Endometriosis
Here Duphaston is taken across most of the cycle rather than just the back half, suppressing womb-lining tissue growing where it should not be. It is one option among several and does not work for everyone — endometriosis rewards honest expectations over optimism.
PMS and painful periods
Second-half-of-cycle dosing targets the mood and physical swing before a period. The evidence here is thinner than for the bleeding indications, and response varies. If Duphaston helps you, it tends to help noticeably; if it does not, persisting for months rarely changes that.
HRT: protecting the womb lining
This one is not about symptoms at all. If you take estrogen for menopause and still have your uterus, estrogen alone can thicken the lining over time — a risk you do not want. Adding a progestogen for part of each cycle prevents that build-up. Dydrogesterone is a common partner for estradiol in combined HRT, and our guide to local estrogen therapy for menopause symptoms covers the other half of that equation.
The Myth That Causes Real Harm
Time to close the loop from earlier. Duphaston is not birth control.
This is the most consequential misunderstanding about Duphaston, and you can see how it arises. Contraceptive pills contain progestogens. Dydrogesterone is a progestogen. The inference feels airtight — and it is wrong.
The reason traces back to that receptor selectivity. Contraceptive progestogens are dosed specifically to suppress ovulation. Duphaston, at the doses used for the conditions above, is not designed to do that job, is not licensed to do it, and is not sold as contraception anywhere. The UK label for a dydrogesterone-containing HRT product spells out the consequence: “Women who may be at risk of pregnancy should be advised to adhere to non-hormonal contraceptive methods.”
In fairness, the science on whether dydrogesterone touches ovulation at all is not perfectly settled — some older work reported partial suppression, and labels in different countries word this differently. But that academic uncertainty does not change the instruction: if pregnancy is a risk you want to avoid, use an actual contraceptive.
Take Sarah, 34 — illustrative, not a real patient. Prescribed Duphaston for irregular cycles, she notices her periods becoming regular and reads that as “the hormones are handling it.” Six weeks later she is pregnant. Nothing malfunctioned. The tablet did exactly what it was prescribed to do, and nothing it was not.
If contraception is what you are actually looking for, that is a different class of medication entirely — our guide to combined contraceptive pills explains how those work, and if you already have some at home, it is worth knowing whether birth control expires.
Duphaston Side Effects and Who Should Avoid It
Duphaston side effects are, for most people, mild and manageable. The receptor selectivity that makes dydrogesterone precise also keeps its side-effect list short. That is not the same as harmless, and the table below uses frequency categories from the UK Summary of Product Characteristics rather than vague “may occur” language.
| Side effect | Frequency | Severity | What to do |
|---|---|---|---|
| Headache or migraine | Common (1 in 100 to 1 in 10) | Mild–moderate | Usually settles. A new or severe migraine warrants a call. |
| Nausea | Common | Mild | Take with food; often fades after the first cycle. |
| Menstrual changes (breakthrough or altered bleeding) | Common | Mild–moderate | Expected early on; persistent or heavy bleeding needs review. |
| Breast pain or tenderness | Common | Mild | Usually settles; mention it if it does not. |
| Dizziness or drowsiness | Uncommon (1 in 1,000 to 1 in 100) | Mild | See how it affects you before driving. |
| Vomiting, oedema, weight gain | Uncommon | Mild–moderate | Raise at your next review if persistent. |
| Allergic reaction or abnormal liver function | Rare | Potentially serious | Stop and seek medical help — rash, swelling, jaundice or severe abdominal pain. |
What is missing from this list is as informative as what is on it. Acne, greasy skin and unwanted hair growth — the complaints that drive people off older progestogens — are not typical here. That is receptor selectivity showing up in lived experience rather than in a diagram.
Pharmacists see one recurring pattern: people stop in the first month because of nausea or breast tenderness, precisely when those effects are most likely to be settling. If the effect is tolerable, giving it a full cycle before judging is the more informative move. If it is not, say so — there are alternatives, and enduring a bad fit silently helps nobody.
What Does the Research Say?
The evidence for Duphaston is strongest where it has been tested head-to-head against the current standard: luteal phase support in IVF. It is weaker, and more contested, in early pregnancy. Both deserve honest treatment.
The LOTUS trials: an oral tablet versus a vaginal gel
The LOTUS programme asked a question with real-world stakes. Vaginal progesterone works, but many people dislike it — discharge and irritation are genuine reasons for poor adherence. Could a tablet do the same job?
LOTUS I randomised 1,031 women across 38 sites to oral dydrogesterone 30 mg daily or micronised vaginal progesterone 600 mg daily, finding the tablet non-inferior at 12 weeks. LOTUS II repeated the exercise against a vaginal gel in 1,034 women across 37 centres, same verdict.
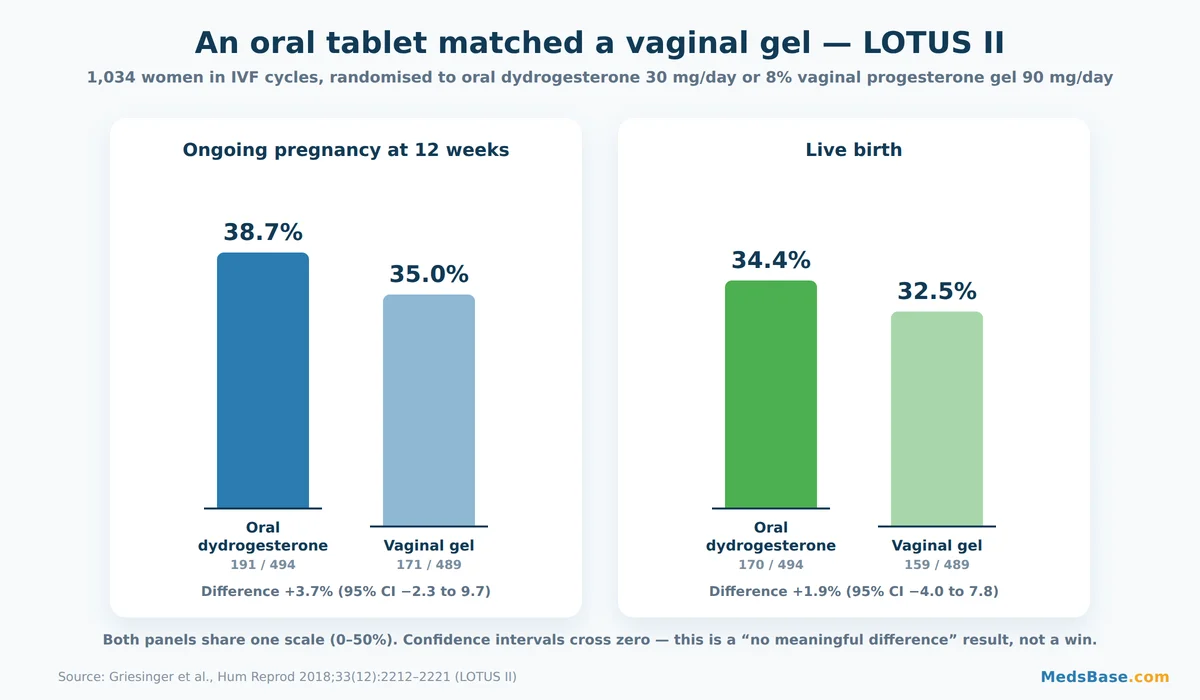
Read those numbers carefully. In LOTUS II, ongoing pregnancy at 12 weeks was 38.7% with the tablet versus 35.0% with the gel; live birth was 34.4% versus 32.5%. Both confidence intervals comfortably cross zero. This is not evidence that Duphaston is better — it is evidence it is not worse, which for a treatment swapping a gel for a tablet is the entire point. The win is convenience, not potency.
Miscarriage: where the evidence gets genuinely murky
This is where most articles quietly mislead, so here is the distinction that matters. The progesterone evidence and the dydrogesterone evidence are not interchangeable.
The two large, famous UK trials — PROMISE and PRISM — tested micronised progesterone, not dydrogesterone. PRISM randomised 4,153 women with early-pregnancy bleeding and found no significant live-birth benefit overall (75% vs 72%), with a signal only in the subgroup who had already had three or more miscarriages. When someone cites PRISM to argue for or against dydrogesterone, they are quoting a trial of a different drug.
Duphaston’s own evidence sits mostly in smaller reviews by Carp, which reported lower miscarriage rates in both threatened miscarriage and recurrent miscarriage. Those results look encouraging — and they rest on a far smaller, more heterogeneous evidence base than PRISM’s 4,153 women. Encouraging is not established.
Worth knowing: miscarriage is not even a licensed use everywhere. The UK label does not list it; other countries’ labels do. That is not a scandal — regulators weigh the same imperfect evidence and reach different conclusions. It is, however, why you will find flatly conflicting information online depending on which country’s page you land on.
The safety question nobody should skip
In 2015, a case-control study by Zaqout and colleagues compared 202 children born with congenital heart disease against 200 without, and reported that their mothers had taken more dydrogesterone in the first trimester (adjusted odds ratio 2.71). That is a frightening headline, and it deserves to be reported rather than buried.
It also deserves context. The study was retrospective, relying on mothers recalling medication use years later — a design vulnerable to recall and selection bias. A 2024 systematic review in Human Reproduction Open excluded it for critical risk of bias. Pooling six randomised trials covering 1,512 live births, it found a risk ratio of 0.92 (95% CI 0.55–1.55) — roughly 35 anomalies per 1,000 with dydrogesterone versus 38 without. Its conclusion: no relevant additional risk.
The honest summary: the larger, better-designed evidence is reassuring — and its authors graded their own certainty as low. That is not a loophole; it is what integrity looks like where trials are smaller than anyone would like. Decisions about hormones in pregnancy belong with your doctor, not an article.
Research summary
| Study | Year | Finding | Source |
|---|---|---|---|
| LOTUS I (Tournaye et al.) | 2017 | Oral dydrogesterone non-inferior to vaginal progesterone in 1,031 women (IVF luteal support) | Hum Reprod |
| LOTUS II (Griesinger et al.) | 2018 | Non-inferior to vaginal gel in 1,034 women; live birth 34.4% vs 32.5% (CI crosses zero) | Hum Reprod |
| Carp systematic review | 2012 | Research suggests lower threatened-miscarriage rate (13% vs 24%); small evidence base | Gynecol Endocrinol |
| Carp systematic review | 2015 | Research suggests lower recurrent-miscarriage rate (10.5% vs 23.5%) across 509 women | Gynecol Endocrinol |
| Zaqout et al. (case-control) | 2015 | Reported association with congenital heart disease (aOR 2.71); later judged critical risk of bias | Pediatr Cardiol |
| Katalinic et al. (meta-analysis) | 2024 | No additional congenital-anomaly risk; RR 0.92 (0.55–1.55) across 6 RCTs; certainty graded low | Hum Reprod Open |
What this means for you: for cycle control, bleeding or HRT, you are on the well-trodden part of the map. In early pregnancy, the evidence is real but limited — a conversation for your doctor, with the uncertainty on the table.
Dydrogesterone vs Progesterone and Other Progestogens
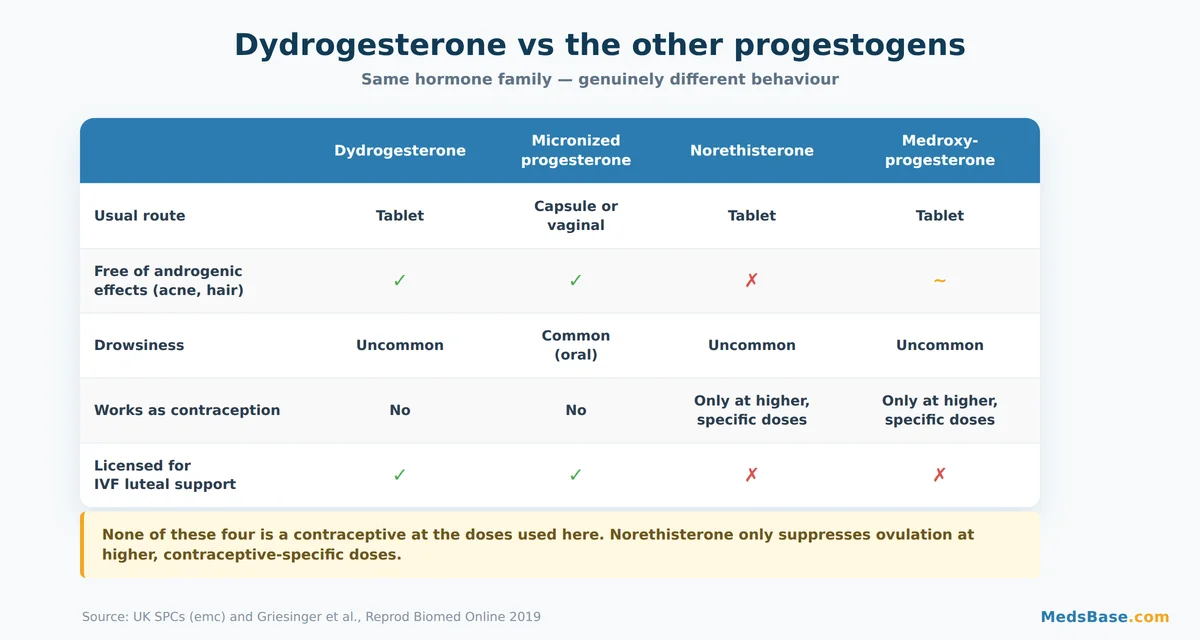
The dydrogesterone vs progesterone question comes up constantly, and the useful answer is not “which is better” but “which trade-off suits you”. These are different tools, not competitors.
| Dydrogesterone | Micronised progesterone | Norethisterone | Medroxyprogesterone | |
|---|---|---|---|---|
| Usual route | Tablet | Capsule or vaginal | Tablet | Tablet |
| Androgenic effects | Not typical | Not typical | Possible (acne, hair) | Weak |
| Drowsiness | Uncommon | Common with oral dosing | Uncommon | Uncommon |
| Works as contraception | No | No | Only at higher, specific doses | Only at higher, specific doses |
| Best suited to | Cycle control, HRT, oral luteal support | Those wanting body-identical hormone | Period delay, heavy bleeding | HRT, bleeding disorders |
Which fits which situation? If you want a body-identical hormone and do not mind vaginal dosing — or would welcome the sedative effect at bedtime — micronised progesterone, such as Susten vaginal gel, makes sense. If you want an oral tablet with minimal androgenic baggage and no drowsiness, Duphaston is the natural pick. If your goal is to delay a period, norethisterone is the tool built for that job — our guide to norethisterone for period delay explains why the two are not interchangeable.
One caveat: “body-identical” carries emotional weight that outruns the evidence. It is a real pharmacological distinction, not proof of superiority. For most indications here, both work.
Duphaston Dosage — How to Take It
Duphaston dosage is where most avoidable failures happen — and almost never because of the number of milligrams. The tablet is 10 mg in every scenario below. What changes is which days of your cycle you take it on, and that is what people get wrong.
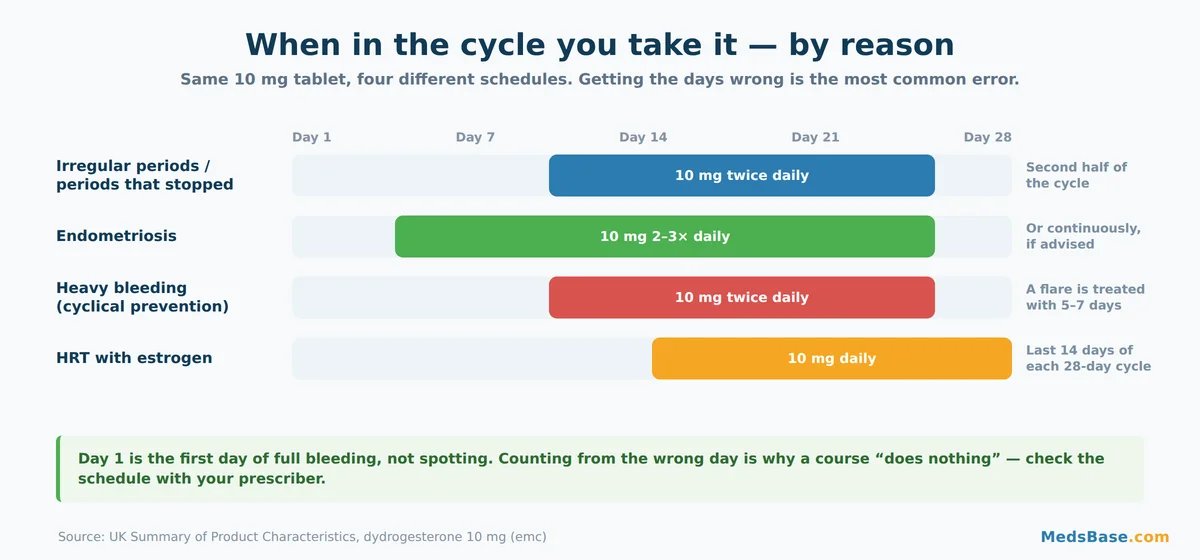
Typical UK Summary of Product Characteristics schedules, for orientation only — yours comes from your prescriber:
- Irregular periods or secondary amenorrhoea: 10 mg twice daily, day 11 to 25, usually with an estrogen.
- Dysfunctional uterine bleeding: 10 mg twice daily for five to seven days to settle an active bleed; day 11 to 25 to prevent recurrence.
- Endometriosis: 10 mg two to three times daily from day 5 to day 25, or continuously.
- HRT with an estrogen: 10 mg daily for the last 14 days of each 28-day cycle; sometimes increased to 20 mg.
Mistakes to avoid
- Miscounting day 1. Day 1 is the first day of full bleeding, not spotting. Start from the wrong day and a course can genuinely appear to do nothing.
- Stopping the moment bleeding settles. Finishing a cyclical course is what produces a controlled withdrawal bleed. Quitting early invites the erratic bleeding back.
- Treating it as a daily-forever tablet. Most schedules are windows, not routines. This is not a blood-pressure pill.
- Assuming you are protected from pregnancy. The error with the largest consequence.
- Ignoring bleeding that does not fit the plan. Early breakthrough bleeding is common; bleeding that is heavy, prolonged or new after months of stability is a reason to be seen.
Take Duphaston 10mg with or without food — if nausea appears, food helps. Miss a dose? Take it when you remember unless the next is close; never double up. On HRT, the progestogen half is not optional garnish: skipping it defeats the reason it was added.
MedsBase stocks Duphaston (dydrogesterone 10 mg) from WHO-GMP-certified manufacturers, with worldwide shipping and no prescription needed.
Why Duphaston Isn’t Sold in the US — and What the FDA Actually Said
Searching for Duphaston from the United States, you hit a wall. It is licensed in more than a hundred countries — the UK, Ireland, Australia, South Africa and much of Asia — yet it is absent from American shelves. The natural inference is that the FDA saw something alarming.
It did not — and there is a document that says so outright.
In September 2017 the FDA published a formal determination in the Federal Register addressing GYNOREST (dydrogesterone) oral tablets, 5 mg and 10 mg — the subject of NDA 017388, approved in October 1978. The finding was unambiguous:
“We have carefully reviewed our files for records concerning the withdrawal of GYNOREST (dydrogesterone) oral tablets, 5 mg and 10 mg, from sale. We have also independently evaluated relevant literature and data for possible post-marketing adverse events. We have found no information that would indicate that this drug product was withdrawn from sale for reasons of safety or effectiveness.“
The Agency went further, noting “dydrogesterone oral tablets are being sold in many other countries,” and classified the product under the Orange Book’s Discontinued Drug Product List — which, in the FDA’s own words, covers drugs discontinued “for reasons other than safety or effectiveness”. You can read the determination in full.
So what happened? The mundane version: US distribution wound down around 1981, and Solvay requested withdrawal of the remaining NDA in 1992 — approval lapsed in July 1993. A commercial retreat, decades ago, in one market, while the drug carried on being prescribed across Europe and Asia.
The distinction to hold onto: “not approved in the US today” and “found unsafe” are different statements, and only the first is true. Equally, the determination is not an approval — do not read it as the FDA endorsing Duphaston. It is duller than that: a finding that safety was never the reason it left.
Related reading
- Primolut N (norethisterone): period delay and heavy bleeding — the progestogen most often confused with this one.
- Diane-35 contraceptive pill guide — what to use when you do want contraception.
- Evalon (estriol) cream guide — the estrogen side of menopause care.
Frequently Asked Questions
What is Duphaston used for?
Duphaston (dydrogesterone 10 mg) is used where your body’s progesterone is insufficient, or where estrogen needs balancing. Licensed uses include irregular periods, secondary amenorrhoea, heavy or prolonged bleeding, endometriosis, painful periods and PMS. It is also added to estrogen in HRT to stop the womb lining thickening unopposed. In some countries it is additionally licensed for threatened or recurrent miscarriage, though the UK label does not include that use.
Is Duphaston a contraceptive?
No. Despite being a progestogen — the same hormone family used in contraceptive pills — dydrogesterone is not licensed or sold as contraception anywhere, and it should never be relied on to prevent pregnancy. The UK label for a dydrogesterone-containing HRT product advises women who may be at risk of pregnancy to use non-hormonal contraceptive methods. If you need contraception, you need a product designed and dosed for that purpose.
Can Duphaston delay your period?
Not reliably, and it is not the right tool for the job. Taking a progestogen and then stopping it typically triggers a withdrawal bleed, so cyclical dydrogesterone tends to regulate when a period arrives rather than postpone one on demand. Norethisterone is the progestogen usually prescribed specifically for period delay, on a different schedule. Ask your prescriber rather than improvising with a tablet you already have.
How long does it take for Duphaston to work?
It depends on the goal. For an active heavy bleed, a short course often settles things within a few days. For cycle regulation, judge it over two or three full cycles rather than one — a single cycle rarely tells you much. For endometriosis or PMS, several months may be needed to know whether it genuinely helps you. If nothing has changed after three cycles, that is worth reviewing rather than pushing through.
Does Duphaston help you get pregnant?
It is not a fertility drug and does not cause ovulation. Where it has a genuine role is luteal phase support during IVF: the LOTUS I and LOTUS II trials found oral dydrogesterone non-inferior to vaginal progesterone for pregnancy and live-birth rates. It may also be used where low progesterone is contributing to difficulty conceiving. Outside those contexts, it will not improve your chances, and any use around pregnancy should be doctor-led.
What are the side effects of Duphaston 10mg?
The common ones — affecting between 1 in 100 and 1 in 10 people — are headache or migraine, nausea, breast tenderness and changes to menstrual bleeding. Less commonly you might notice vomiting, dizziness, drowsiness, mild swelling or weight gain. Rarely, allergic reactions or abnormal liver function occur; those need prompt medical attention. Notably, acne and unwanted hair growth are not typical, unlike with some older progestogens.
Is dydrogesterone safe in early pregnancy?
The best current evidence is reassuring but not conclusive. A 2015 case-control study reported a link with congenital heart disease, but it was retrospective and later judged to carry a critical risk of bias. A 2024 meta-analysis of six randomised trials covering 1,512 live births found no additional risk of congenital anomalies (RR 0.92), while grading its own certainty as low. Any use in pregnancy is a decision for your doctor.
Why can’t I buy Duphaston in the United States?
Because it was commercially withdrawn decades ago, not because it was found unsafe. The FDA stated in a 2017 Federal Register determination that it found no information indicating the product was withdrawn from sale for reasons of safety or effectiveness, and noted that dydrogesterone tablets are sold in many other countries. It sits on the Orange Book’s Discontinued Drug Product List — reserved for drugs discontinued for reasons other than safety or effectiveness.
The Bottom Line
Duphaston is a well-established, unusually clean progestogen. Its mirrored structure buys two real advantages: it works as a tablet, and it largely avoids the androgenic side effects that drive people off other progestogens. For cycle control, heavy bleeding and HRT lining protection, it rests on decades of use and a clear mechanism. In IVF luteal support it matched vaginal progesterone in two trials of over a thousand women each. In early pregnancy the evidence is real but thin.
The two things most worth carrying away are both correctives. It is not contraception — if pregnancy is a risk you want to avoid, use something built for that. And its absence from US shelves is a commercial artefact, not a safety verdict — the FDA put that in writing.
If you take one action today: find out which cycle days your schedule actually specifies, and check you are counting day 1 from full bleeding rather than spotting. That single detail decides whether a course works more often than the dose does.
Wondering how this compares to the progestogen used for delaying a period instead of regulating one? Read our norethisterone guide. Trying to work out where hormone therapy fits into menopause care more broadly? Start with our women’s health range and talk the options through with a qualified healthcare provider before you commit to any of them.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.