







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Antibiotics and yeast infections are one of the most common medicine-related complaints in women’s health — and one of the most misunderstood. You take an antibiotic to clear a chest or urine infection, and days later you notice itching, burning, and a thick white discharge. It feels like the cure caused a new problem, and in a sense it did.
The good news: this reaction is well understood, usually mild, and preventable. This guide explains exactly why the link between antibiotics and yeast infections happens, which antibiotics carry the highest risk, how to tell a true yeast infection from look-alike conditions, and the evidence behind prevention steps like probiotics. Everything here is written to help you act sensibly, not to alarm you.
- Broad-spectrum antibiotics (like amoxicillin and tetracyclines) raise yeast-infection risk the most; narrow-spectrum drugs raise it least.
- The antibiotic does not create Candida — it removes the protective bacteria that normally hold existing yeast in balance.
- Only a minority of people who take antibiotics develop symptomatic thrush; most never notice a thing.
- Symptoms typically appear during the course or within a week of finishing it.
- A single-dose or short-course antifungal usually clears it; recurring cases deserve a clinician’s review.
- Not every post-antibiotic discharge is yeast — bacterial vaginosis and STIs can mimic it and need different treatment.
What Is the Link Between Antibiotics and Yeast Infections?
A yeast infection after antibiotics is an overgrowth of the fungus Candida — usually Candida albicans — that occurs when antibiotics wipe out the friendly bacteria keeping it in check. The vagina, mouth, and gut all rely on that bacterial balance, so the yeast can flare in any of them.
Understanding antibiotics and yeast infections starts with one fact: Candida already lives on and inside most healthy people. According to MedlinePlus, small amounts of this yeast are a normal part of the vaginal environment. It only becomes a problem when something disturbs the balance that keeps it quiet — and a course of antibiotics is one of the classic triggers.
This is why the reaction feels so unfair. The antibiotic is doing its job against harmful bacteria, but it cannot tell friend from foe. When the protective bacteria fall, the yeast that was already present has room to multiply. The result is a vaginal yeast infection (or oral thrush) that seems to appear out of nowhere.
Importantly, the connection between antibiotics and yeast infections is common but not universal. Most people finish a course of antibiotics with no yeast trouble at all. Whether you develop symptoms depends on the drug, its spectrum, how long you take it, and your own biology.
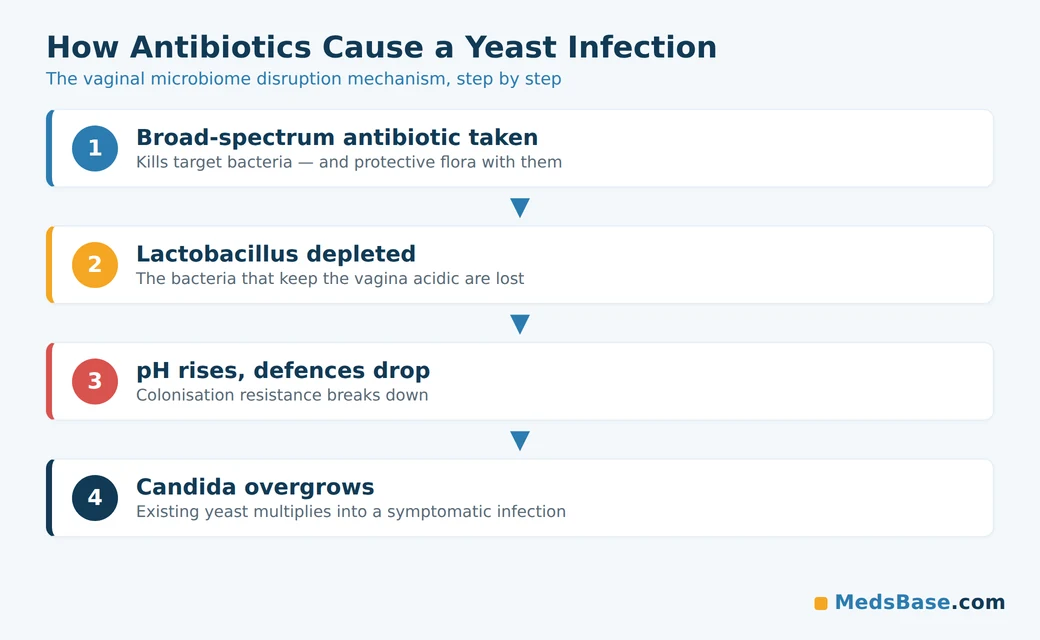
How Do Antibiotics Cause Yeast Infections? The Microbiome Mechanism
Antibiotics cause yeast infections indirectly: they kill the Lactobacillus bacteria that keep the vagina acidic and hostile to Candida. With those bacteria gone, vaginal pH drifts up, competition for space disappears, and the yeast overgrows into a symptomatic infection.
Here is the chain of events in plain English. A healthy vagina is dominated by Lactobacillus species. These bacteria produce lactic acid, which keeps the pH low (around 3.8–4.5), plus hydrogen peroxide and other compounds that suppress yeast and unwanted microbes. That acidic, competitive environment is called colonisation resistance — the microbiome’s built-in defence.
Broad-spectrum antibiotics do not target Candida (antibiotics do not kill fungi at all). Instead they deplete the Lactobacillus population as collateral damage. Once the guardians are gone, three things shift at once: the pH rises, the physical space frees up, and the chemical signals that held the yeast back disappear. Candida, already present in low numbers, seizes the opening.
The same mechanism behind antibiotics and yeast infections explains oral thrush and, less often, skin or nappy-area yeast. Wherever antibiotics disturb the local bacterial balance, opportunistic Candida can move in. That is why understanding how antibiotics cause yeast infections matters more than memorising a drug list — the principle is always the same.
Which Antibiotics Are Most Likely to Cause Thrush?
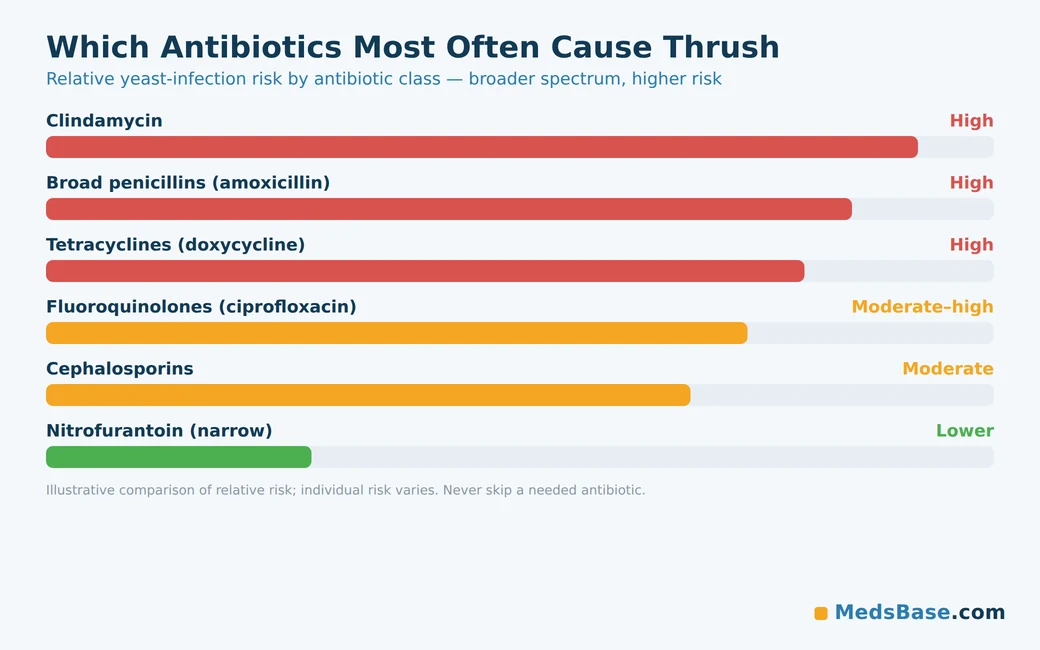
When it comes to antibiotics and yeast infections, the spectrum of the drug matters most. Broad-spectrum antibiotics — those that kill a wide range of bacteria — are the most likely to cause thrush, because they do the most collateral damage to protective flora. Narrow-spectrum antibiotics that target a specific bug tend to spare more of the good bacteria and carry lower risk.
Higher-risk antibiotic classes
These broad-spectrum drugs disturb the most bacteria and are most often linked to yeast overgrowth:
- Penicillins — amoxicillin and amoxicillin-clavulanate, common for chest, ear, sinus and dental infections.
- Tetracyclines — doxycycline and related drugs, often used long-term for acne, which lengthens the exposure.
- Cephalosporins — such as cephalexin, used for skin and urinary infections.
- Fluoroquinolones — such as ciprofloxacin, broad and potent.
- Clindamycin — strongly linked to gut and vaginal flora disruption.
Lower-risk antibiotic choices
Narrow-spectrum agents are less likely to cause thrush because they leave more protective bacteria intact. Nitrofurantoin, for example, is often chosen for simple urine infections partly because it concentrates in the bladder and disturbs less elsewhere. Choosing the narrowest effective antibiotic is a core principle of responsible prescribing, as explained by the NHS antibiotics guidance.
Two practical points follow. First, longer courses raise cumulative risk, which is why acne patients on months of doxycycline notice thrush more often. Second, the answer to antibiotics and yeast infections is never to skip a genuinely needed antibiotic — it is to use the right one for the right duration. If you want to understand how different agents compare, our overview of the most widely used antibiotics and the wider antibiotics range put the options in context.
Yeast Infection Symptoms, Timing and Severity
Recognising the symptoms is the practical heart of dealing with antibiotics and yeast infections. A post-antibiotic yeast infection usually announces itself with intense itching, a thick white discharge, and redness. Symptoms often begin during the antibiotic course or within a few days of finishing, and most cases are uncomfortable rather than dangerous.
The classic signs of a vaginal yeast infection include vulval itching and burning, a thick white “cottage cheese” discharge that usually has little odour, soreness or swelling, discomfort during sex, and stinging when you pass urine. Oral thrush instead shows up as white patches inside the mouth and a sore tongue. The NHS overview of thrush describes the same pattern.
The table below summarises how common each symptom is and how seriously to take it. Frequency labels are general patterns, not guarantees — your experience may differ.
| Symptom | How common | Severity & action |
|---|---|---|
| Vulval itching & burning | Very common | Mild–moderate; usually responds to antifungal treatment |
| Thick white discharge | Very common | Mild; a hallmark sign, low odour |
| Redness & swelling | Common | Mild–moderate; soothed as infection clears |
| Pain during sex or urination | Common | Moderate; treat promptly for comfort |
| Oral white patches (thrush) | Less common | Moderate; more likely in infants, elderly, inhaler users |
| Fever or spreading illness | Rare | Serious; seek medical care — this is not typical thrush |
Most yeast infections triggered by antibiotics are self-limited and easily treated. Warning signs that call for professional help include a first-ever episode you are unsure about, symptoms in pregnancy, four or more episodes a year, no improvement after treatment, or any fever and feeling unwell. For skin folds and nappy-area candidiasis, a topical option such as Candid B antifungal cream is commonly used.
What Does the Research Say About Antibiotics and Yeast Infections?
Research consistently supports a real but modest link. On antibiotics and yeast infections, studies show antibiotics raise Candida colonisation and the chance of symptomatic thrush, though most courses pass without incident. Evidence for prevention with probiotics is promising but still limited and mixed.
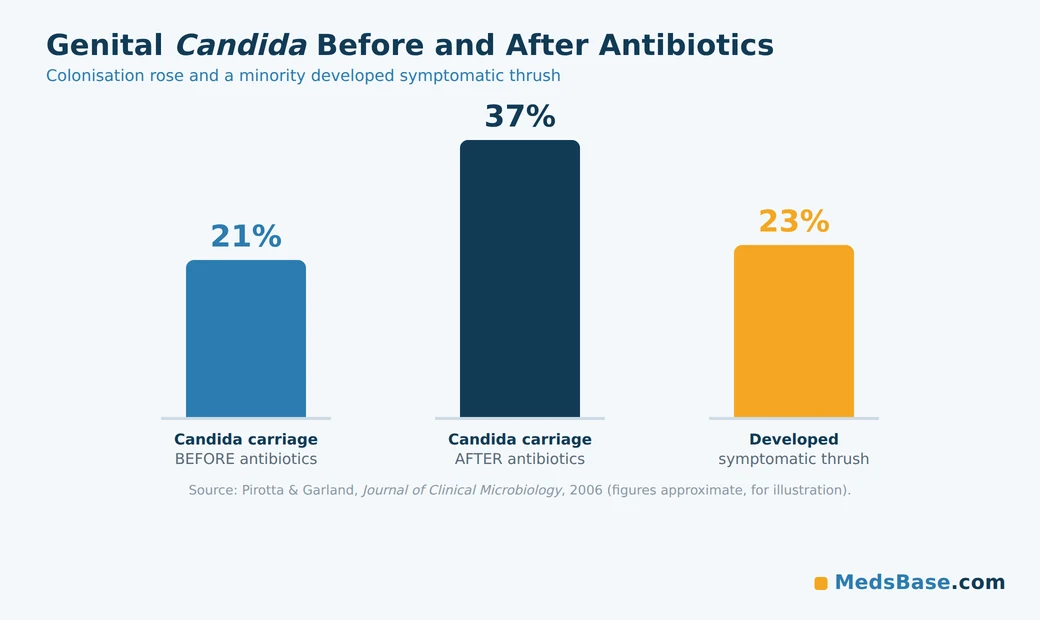
The clearest human data on antibiotics and yeast infections comes from before-and-after sampling studies. These consistently show yeast levels climbing after a broad-spectrum course, with a subset of people developing symptoms. The table below summarises key findings, using cautious language because individual risk varies widely.
| Source | Year | What it suggests | Reference |
|---|---|---|---|
| Pirotta & Garland, J. Clin. Microbiol. | 2006 | Genital Candida colonisation rose after antibiotics; a minority developed symptomatic thrush. | PubMed |
| MedlinePlus (NIH/NLM) | Current | Antibiotic use is listed among the recognised triggers of vaginal yeast infections. | MedlinePlus |
| Office on Women’s Health | Current | Names antibiotics, pregnancy, diabetes and immune suppression as key risk factors. | womenshealth.gov |
| Probiotic prevention reviews | Recent | Low-certainty evidence of modest benefit; better trials are still needed. | See guidance |
Two honest caveats belong here. First, “antibiotics raise the risk” does not mean “antibiotics guarantee an infection” — the majority of courses cause no thrush. Second, prevention research is thinner than people assume: while Lactobacillus probiotics are biologically logical, the trial evidence for preventing antibiotic-associated yeast infections is limited and of low certainty. Early studies indicate possible benefit, but the science is not settled.
Antibiotic-Associated Thrush vs Other Vaginal Infections
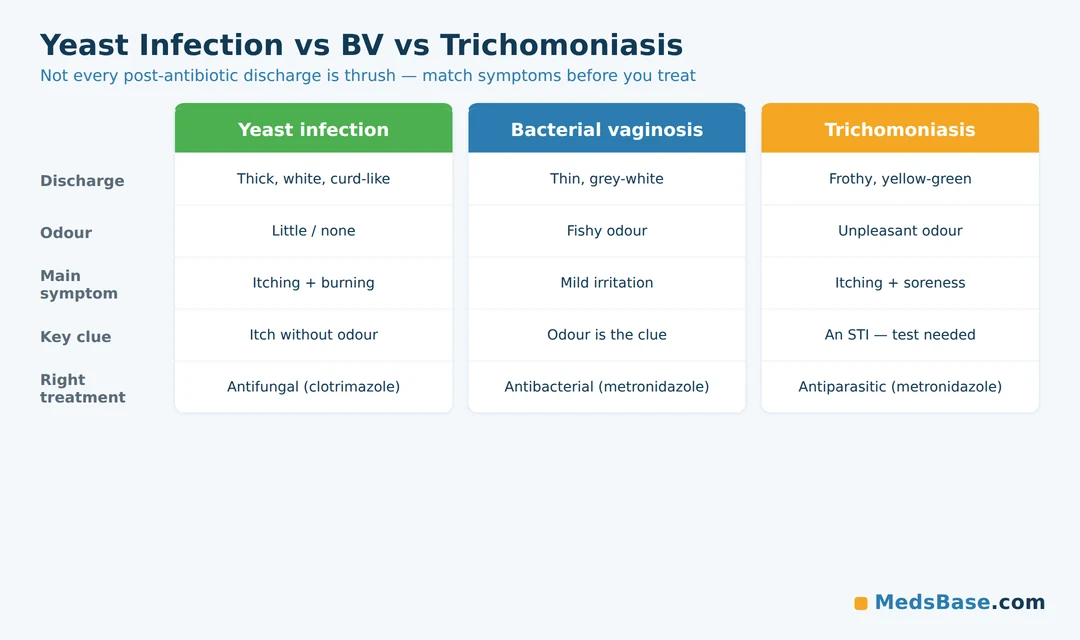
One of the biggest mistakes people make with antibiotics and yeast infections is assuming every symptom is thrush. Not every discharge after antibiotics is a yeast infection. Bacterial vaginosis (BV) and trichomoniasis can look similar but need completely different treatment — antifungals will not touch them. Telling them apart before you treat saves time and money.
This is the single most useful section of this guide, because self-diagnosis errors are common. A true yeast infection responds to antifungals; BV and trichomoniasis respond to antibacterial or antiparasitic drugs. Treating the wrong one delays relief. The comparison below highlights the practical differences.
| Feature | Yeast infection | Bacterial vaginosis | Trichomoniasis |
|---|---|---|---|
| Discharge | Thick, white, “cottage cheese” | Thin, grey-white | Frothy, yellow-green |
| Odour | Little or none | Fishy, especially after sex | Unpleasant |
| Main symptom | Itching, burning | Odour, mild irritation | Itching, soreness |
| Right treatment | Antifungal (e.g. clotrimazole) | Antibacterial (e.g. metronidazole) | Antiparasitic (metronidazole) |
If your symptoms match the BV column — thin discharge with a fishy odour rather than itching — an antifungal will not help, and you can read more in our guide to bacterial vaginosis treatment. If there is any chance of a sexually transmitted infection, or you simply are not sure, testing before treating is the sensible route. When the picture clearly fits yeast, though, antifungal treatment is straightforward.
How to Prevent and Treat a Yeast Infection From Antibiotics
Managing antibiotics and yeast infections comes down to two goals: clear any active infection quickly, and protect your microbiome next time. To treat a yeast infection from antibiotics, use a short-course or single-dose antifungal such as clotrimazole or fluconazole. To prevent one, take antibiotics only when truly needed, finish the correct course, and consider probiotics and simple hygiene measures alongside them.
Treating an active infection
Most uncomplicated yeast infections clear with a topical azole antifungal — for example a clotrimazole vaginal gel used for a few nights — or a single oral fluconazole dose. These options are widely available without a prescription, and you can compare formats in our roundup of the most effective antifungal treatments or browse the full fungal-infection treatment range. Relief usually begins within a couple of days; if it does not, reassess the diagnosis.
Preventing one during your next course

Prevention is largely about protecting your microbiome while the antibiotic does its job — the key to breaking the antibiotics and yeast infections cycle. The most evidence-aligned steps are:
- Only take antibiotics when they are genuinely needed. Skipping unnecessary courses is the most reliable prevention of all.
- Use the narrowest effective antibiotic for the shortest correct duration — a conversation worth having with your prescriber.
- Consider a Lactobacillus probiotic during and after the course. Evidence is modest, but a quality multi-strain probiotic is low-risk and may help restore balance.
- Keep the area cool and dry — breathable cotton underwear and avoiding harsh soaps or douching, which further disturb flora.
- Manage blood sugar if you have diabetes, since high glucose feeds yeast.
- Have antifungal treatment on hand if you are prone to post-antibiotic thrush, so you can act at the first sign.
People with recurrent antibiotic-associated yeast infections sometimes ask their clinician about taking a preventive antifungal dose alongside the antibiotic. That is a reasonable individualised discussion, but it is not something to self-prescribe routinely. For general women’s-health support and related products, our women’s health hub is a useful starting point.
Restoring your microbiome after the course
Prevention does not stop the day your tablets run out. The protective bacteria take time to recover, so the window for a late yeast flare can last a week or two beyond the final dose. Continuing a probiotic through that recovery period is a sensible, low-risk habit, and spacing it a couple of hours apart from any remaining antibiotic dose helps the live cultures survive.
Everyday choices support the rebuild too. Fermented foods, adequate hydration, and steady blood-sugar control all favour a Lactobacillus-dominant balance. There is no need to obsess over “detoxes” or expensive regimens — the microbiome is resilient, and most people return to normal on their own. The aim is simply to avoid piling on extra disruptions while it recovers, which is where the practical side of managing antibiotics and yeast infections really pays off.
Special Situations: Pregnancy, Diabetes and Recurring Thrush
Some groups face a higher or more complicated risk when antibiotics and yeast infections combine — notably pregnant women, people with diabetes, and anyone with recurrent thrush. The general advice still applies, but treatment choices and follow-up need a little more care in these situations.
Pregnancy
Yeast infections are more common in pregnancy because hormonal changes shift the vaginal environment, and antibiotics can add to that. Treatment is still possible, but the choice matters: topical clotrimazole is generally preferred over oral fluconazole during pregnancy. If you are pregnant and suspect a yeast infection after antibiotics, confirm it with your midwife or doctor rather than self-treating, because some look-alike infections carry their own risks in pregnancy.
Diabetes and blood sugar
High blood glucose feeds Candida, so people with diabetes tend to get yeast infections more easily and more often — and a course of antibiotics can be the final trigger. Keeping blood sugar well controlled is one of the most effective, and most overlooked, ways to lower the risk. If you notice a pattern of thrush after antibiotic courses, review both your glucose control and your antibiotic choices with your care team.
Recurrent yeast infections
Four or more yeast infections in a year is defined as recurrent vulvovaginal candidiasis, and it deserves a proper work-up rather than repeated guesswork. When antibiotics and yeast infections seem to go hand in hand every single time, a clinician may recommend a longer or maintenance antifungal plan, confirm the exact species involved, and look for underlying contributors. Repeated self-treatment without a diagnosis is the most common reason thrush keeps returning.
Oral thrush, inhalers and babies
The mouth has its own microbiome, so broad-spectrum antibiotics can also cause oral thrush — white patches, soreness, and altered taste. It is more likely in babies, older adults, denture wearers, and people using steroid inhalers. Rinsing the mouth after inhaler use and keeping up good oral hygiene lower the risk. In infants, oral thrush and antibiotic-related nappy-area yeast often appear together and usually respond well to gentle antifungal treatment.
- “Everyone gets thrush from antibiotics.” Not true — most people do not. Risk depends on the drug, the dose, the duration, and your own biology.
- “The antibiotic gave me the yeast.” The yeast was already present; the antibiotic simply removed the bacteria that were keeping it quiet.
- “Any discharge after antibiotics must be thrush.” Bacterial vaginosis and other causes can mimic it and need different treatment — so match the symptoms before you treat.
Frequently Asked Questions
Q: Why do antibiotics cause yeast infections?
A: Antibiotics cause yeast infections indirectly. They kill the protective Lactobacillus bacteria that keep the vagina acidic and crowd out yeast. Once those bacteria fall, the pH rises and the Candida already living there overgrows into a symptomatic infection. The antibiotic never targets the yeast itself — it simply removes the competition that normally keeps it under control, which is why broad-spectrum drugs cause the most trouble.
Q: How long after antibiotics does a yeast infection start?
A: Symptoms usually begin during the antibiotic course or within a few days to a week of finishing it. That timing reflects how quickly protective bacteria are depleted and how fast yeast can multiply once the balance tips. If itching and discharge appear more than two weeks after your last dose, another cause is more likely, and it is worth getting checked rather than assuming it is antibiotic-related thrush.
Q: Which antibiotics are most likely to cause thrush?
A: Broad-spectrum antibiotics carry the highest risk — penicillins such as amoxicillin, tetracyclines such as doxycycline, cephalosporins, fluoroquinolones, and clindamycin. They disturb the widest range of bacteria, including the protective ones. Narrow-spectrum antibiotics like nitrofurantoin generally cause less thrush because they spare more of the good flora. Longer courses, such as months of doxycycline for acne, add to the cumulative risk.
Q: Can I take an antifungal at the same time as my antibiotic?
A: Often yes. Antifungals such as clotrimazole and fluconazole work on fungi, while antibiotics work on bacteria, so they do not cancel each other out. People prone to post-antibiotic thrush sometimes treat at the first symptom, or discuss a preventive dose with a clinician. Always check for interactions with your other medicines, and speak to a pharmacist or doctor before combining treatments, especially in pregnancy.
Q: Do probiotics stop yeast infections from antibiotics?
A: They might help, but the evidence is limited. The idea is sound — Lactobacillus probiotics aim to replace the bacteria antibiotics destroy. Some studies suggest a modest protective effect, while others are inconclusive, so the science is not settled. Because a good multi-strain probiotic is low-risk, many people take one during and after a course as a sensible precaution rather than a guaranteed fix.
Q: Is a yeast infection after antibiotics contagious?
A: A yeast infection is not classed as a sexually transmitted infection, and it is not considered contagious in the usual sense. Candida is already present in most people. Occasionally partners can pass yeast back and forth, and a male partner may get mild irritation, but routine partner treatment is not usually needed unless they have symptoms. If symptoms recur or a partner is affected, a clinical review is worthwhile.
Q: When should I see a doctor about antibiotics and yeast infections?
A: See a clinician if it is your first suspected yeast infection, if you are pregnant, if you get four or more episodes a year, if treatment does not work within a week, or if you have fever or feel unwell. These situations need confirmation of the diagnosis and sometimes a longer treatment plan. Recurrent thrush in particular deserves a proper assessment rather than repeated self-treatment.
The Bottom Line
The connection between antibiotics and yeast infections is real, well understood, and manageable. Broad-spectrum antibiotics can tip the microbiome out of balance and let Candida overgrow, but only a minority of people are affected, and a simple antifungal usually restores comfort quickly. The smartest approach to antibiotics and yeast infections is prevention through sensible antibiotic use, plus knowing how to tell true thrush from its look-alikes.
If you are dealing with a post-antibiotic yeast infection now, a proven antifungal treatment is the direct route to relief — and no prescription is needed to get started. Keep this guide handy for your next antibiotic course, and you will know exactly what to watch for and how to respond.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.