







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

About 1 in 8 American adults has now taken a GLP-1 medicine like semaglutide, and most of them inject it themselves at home — once a week, year after year. Yet a huge number of users never get a clear answer to the same first-day question: where on my body should the needle actually go? The instruction leaflet says “abdomen, thigh or upper arm” and stops there.
This guide fixes that. We’ll walk through the three approved semaglutide injection sites — stomach, thigh and upper arm — with diagrams of where each one sits, how they compare on comfort and absorption, and why rotating between them protects your skin. You’ll also find a practical 4-week rotation schedule, a step-by-step injection technique, and answers to the questions most people search for after their first dose.
Key Takeaways
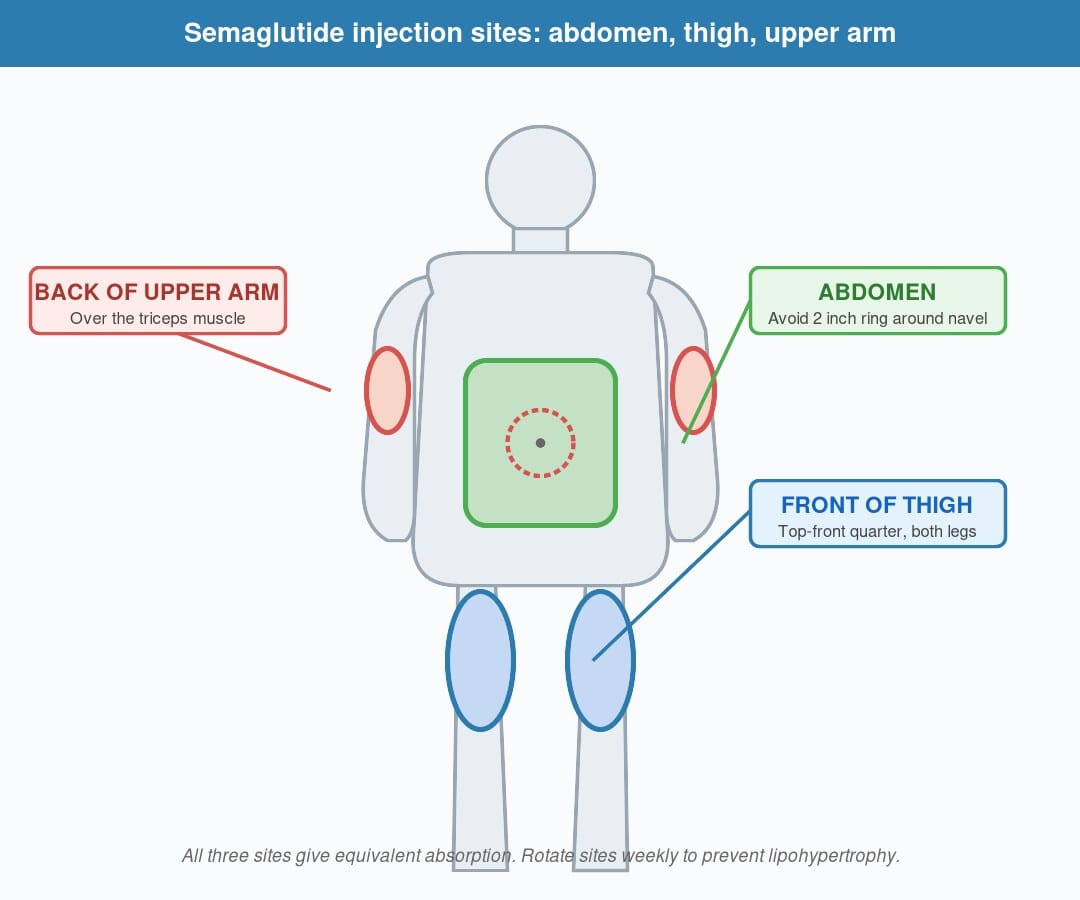
- Semaglutide is approved for subcutaneous injection in three sites: the abdomen (avoiding a 2-inch ring around the navel), the front of the thigh, and the back of the upper arm.
- All three sites give equivalent absorption — there is no “stronger” site.
- Rotating between sites prevents lipohypertrophy (lumpy fat deposits) and reduces local irritation.
- The abdomen is the most popular site for self-injection because it’s easy to see and pinch.
- The upper arm usually requires a helper, since the back of your own arm is hard to reach.
- Pen technique matters more than location: a clean site, a fresh needle, and a 90° insertion angle determine comfort.
Reviewed by Morgan Ellis, Clinical Pharmacy Editor · Last updated: 15 May 2026
Jump to: What is semaglutide? · How it works · The 3 sites · Side effects · The research · Comparison · How to inject · FAQs · Bottom line
What is semaglutide injection?
Semaglutide is a once-weekly injectable medicine in the GLP-1 (glucagon-like peptide-1) receptor agonist class, used to lower blood sugar in type 2 diabetes (brand name Ozempic) and to support long-term weight management (brand name Wegovy). A daily oral tablet form (Rybelsus) also exists, but the injection form is by far the most common because it offers a flatter, more predictable concentration in the bloodstream.
The injection itself is subcutaneous, meaning it goes into the layer of fatty tissue just under the skin — not into a vein and not into a muscle. That layer is shallow, only a few millimetres deep on most people, which is why the needles used for semaglutide pens are very fine and only about 4–8 mm long.
Subcutaneous tissue is well-suited to slow-release medicines. The fat layer acts like a small reservoir: the medication seeps out gradually into nearby capillaries, then binds to a transport protein in the blood called albumin. That binding step is what gives semaglutide its ~7-day half-life — and why one weekly dose is enough.
Quick definition: Semaglutide injection sites are the three areas of the body — abdomen, front of thigh and back of upper arm — where a once-weekly semaglutide injection can be given. All three sites are bioequivalent, so the choice depends on comfort, body composition and rotation rather than potency.
How does semaglutide work after injection?
Once the semaglutide molecule is deposited in subcutaneous fat, it doesn’t rush into the bloodstream. Instead, several things happen in sequence over the following hours and days:
- The drug disperses into nearby tissue and is gradually picked up by tiny capillaries.
- Semaglutide molecules bind to albumin, the most abundant protein in human blood.
- Albumin transports the drug around the body, releasing it slowly to the GLP-1 receptors on the pancreas, brain and stomach.
- At those receptors, semaglutide does three things that drive its effect: it boosts insulin release when blood sugar is high, slows gastric emptying so meals feel filling for longer, and acts on appetite centres in the hypothalamus to reduce food cravings.
Because of the albumin-binding step, the medicine clears from your system very slowly — peak concentration is reached around 24–48 hours after the injection, and useful concentration is maintained for a full week. This is the pharmacological reason your injection site choice matters less for semaglutide than it would for a fast-acting drug like mealtime insulin.
🔬 Research Spotlight
Pharmacokinetic data submitted to the FDA for semaglutide showed no clinically meaningful difference in exposure (AUC) or peak concentration (Cmax) between abdomen, thigh and upper arm injection. The relative bioavailability ratios fell inside the 0.80–1.25 bioequivalence window for all three sites. Source: Ozempic (semaglutide) FDA Prescribing Information, Section 12.3 — Clinical Pharmacology.
The takeaway: the site doesn’t change how much of the dose reaches your system. The site only changes how comfortable, convenient and skin-friendly the injection is for you over months and years of use.
The three approved semaglutide injection sites — with diagram
Semaglutide pens (Ozempic, Wegovy and their WHO-GMP certified generic equivalents) are approved for injection in three anatomical zones. Below is a visual map of where each one sits, plus the pros and cons real users report.
Site 1 — Abdomen (the stomach)
Who is this for? The abdomen is the default site for most self-injectors, and the one diabetes educators recommend first. It’s easy to see, easy to pinch, and easy to rotate within.
Where exactly: any flat area on the front of your abdomen, at least 2 inches (5 cm) away from your belly button in any direction. The shaded ring of skin around the navel is too vascular and uneven for consistent absorption. Avoid scars, stretch marks, moles and any area with visible bruising.
Pros:
- Easiest to reach with your dominant hand
- Largest available surface — lots of room for rotation
- Subcutaneous fat is usually most generous here, even on lean users
- You can see exactly where the needle goes
Cons:
- Some users find this site emotionally uncomfortable if they associate their abdomen with body-image concerns
- Tight waistbands can press on the recent injection site
- After a meal, the abdomen may feel more tender — many users prefer to inject in a fasted state
Site 2 — Front of the thigh
Who is this for? Users who don’t have much abdominal fat, athletes, and people who want to alternate sites without exposing their stomach. The thigh is also a good fall-back when the abdomen is healing from a previous injection.
Where exactly: the front and slightly outer area of the upper thigh — roughly the top half between the hip and the knee. Imagine dividing your thigh into four quarters lengthwise; use the top-front quarter. Avoid the inner thigh (more nerves, more lymph vessels) and avoid right above the kneecap.
Pros:
- Easy to reach while seated
- Comfortable for users who feel anxious about an abdominal needle
- Good option if your abdomen is sensitive after meals
Cons:
- Very lean users may have less subcutaneous fat here — pinching becomes harder
- Walking immediately after the injection may make the area feel sore
- Local redness or itching is sometimes more visible on the thigh
Site 3 — Back of the upper arm
Who is this for? Users with a helper at home, or those who have built up irritation at the other two sites. The upper arm is a fully approved site — but doing it on yourself is awkward for almost everyone.
Where exactly: the back of the upper arm, in the soft tissue over the triceps muscle, roughly halfway between the shoulder and elbow. The skin here should be pinchable — if you can’t pinch at least 1 cm of tissue, choose a different site.
Pros:
- Useful for rotation if abdomen and thigh need a rest
- Less in-the-way during clothing and waistband pressure
- Good for users who don’t want a visible injection site (winter sleeves cover it)
Cons:
- Hard to self-inject — most users need someone to help
- The pinch can be inconsistent if your arm is muscular and lean
- Easier to nick a small surface vessel here

Semaglutide injection safety, side effects and dose
The medication itself has well-documented side effects — mostly gastrointestinal — but this section focuses on injection-site reactions, which are the issues directly affected by where and how you inject.
Injection-site reactions: what’s normal, what isn’t
| Reaction | Typical frequency | Severity | What to do |
|---|---|---|---|
| Mild redness at site | Common (10–15%) | Low | No action; resolves in 24–48 hours |
| Itching at site | Common (5–10%) | Low | Avoid scratching; cool compress if needed |
| Small bruise | Common | Low | Press the area for 10 sec after withdrawal next time |
| Soreness / tenderness | Occasional | Low | Rotate to a different site for next week’s dose |
| Small lump under skin (lipohypertrophy) | Uncommon | Moderate | Stop using that exact spot for 4–6 weeks |
| Persistent rash, swelling or fever | Rare | High | Stop and consult a clinician — may indicate allergy or infection |
| Wheezing, throat tightness, full-body rash | Rare | Serious | Seek immediate emergency care — possible anaphylaxis |
The first four reactions on this list are common, usually mild, and don’t require stopping the medication. The bottom two are not “injection-site” issues — they’re systemic and warrant medical review.
Dosing reminders
Semaglutide is titrated upward slowly to reduce gastrointestinal side effects. A typical schedule:
- Weeks 1–4: 0.25 mg once weekly (starter dose, no clinical effect expected)
- Weeks 5–8: 0.5 mg once weekly
- Weeks 9–12: 1.0 mg once weekly
- Maintenance: 1.0 mg, 1.7 mg or 2.0 mg once weekly (Ozempic) or up to 2.4 mg (Wegovy)
For a full breakdown of pen clicks per dose, see our Ozempic dosage chart guide.
What does the research say?
Three areas have been studied in detail: bioequivalence across sites, lipohypertrophy risk from poor rotation, and injection-site reaction frequency.
| Study / source | Year | Finding |
|---|---|---|
| Ozempic FDA Prescribing Information (Section 12.3) | Updated annually | Semaglutide AUC and Cmax bioequivalent across abdomen, thigh and upper arm |
| SUSTAIN-1 to SUSTAIN-7 (Novo Nordisk) | 2017–2019 | Injection-site reactions in 1–3% of users across all three sites |
| STEP-1 (Wilding et al., NEJM) | 2021 | Subcutaneous injection safety profile consistent across sites |
| Cochrane review on lipohypertrophy (insulin literature, applied by analogy) | 2020 | Site rotation reduces lipohypertrophy risk by >50% versus same-site repeat injection |
| EMA Ozempic SmPC, Section 4.2 | Current | Confirms equivalence and recommends rotation within each anatomical zone |
Research evidence consistently suggests three things:
- The site does not change semaglutide exposure to a meaningful degree.
- Rotation reduces tissue complications — both visible (bruising, lumps) and absorption-related.
- Most injection-site issues are technique-related, not site-related — needle angle, needle reuse and post-injection pressure matter more than which body zone you chose.
Semaglutide vs the alternatives — injection-site comparison
If you’re switching between GLP-1 drugs, the approved injection sites and pen mechanics differ slightly. Here’s how they compare:
| Drug | Approved sites | Frequency | Rotation needed? |
|---|---|---|---|
| Semaglutide (Ozempic, Wegovy) | Abdomen, thigh, upper arm | Weekly | Yes — within and between sites |
| Tirzepatide (Mounjaro, Zepbound) | Abdomen, thigh, upper arm | Weekly | Yes — same principle |
| Liraglutide (Victoza, Saxenda) | Abdomen, thigh, upper arm | Daily | Critical — daily injections compound site stress |
| Dulaglutide (Trulicity) | Abdomen, thigh, upper arm | Weekly | Yes |
| Insulin glargine (Lantus) | Abdomen, thigh, upper arm, buttock | Daily | Critical |
Note that all GLP-1 agonist injectables share the same three approved sites. The differences are in dosing frequency and pen format, not in anatomy. For a closer look at the molecules themselves, see our tirzepatide vs semaglutide comparison.
How to inject semaglutide — step by step
This is the technique that affects comfort more than site selection. Six steps:
- Wash and prepare. Wash your hands with soap and warm water for at least 20 seconds. Lay out a clean surface: the pen, a fresh needle, an alcohol swab and a sharps disposal container.
- Inspect the pen. Hold the semaglutide pen up to the light. The solution inside should be clear and colourless. If you see particles, cloudiness or discolouration, do not use that pen.
- Attach a new needle. Always use a new sterile needle for every dose. Reusing a needle dulls the tip and dramatically increases pain and skin trauma. Twist the new needle on, remove the outer cap (keep this — you’ll use it for safe removal) and the inner cap.
- Prime the pen. Dial 1 unit (or whatever the manufacturer specifies as the “flow check” amount). Hold the pen with the needle pointing up and press the injection button. A drop of liquid should appear at the needle tip. If not, repeat once.
- Dial your dose, choose your site, inject. Dial in your prescribed weekly dose. Choose today’s site according to your rotation plan. Wipe the skin with the alcohol swab and let it air-dry — wet alcohol stings. Pinch a fold of skin lightly, insert the needle at a 90-degree angle, then press the injection button fully.
- Hold, withdraw, dispose. Hold the needle in place for at least 6 seconds after pressing the button — this gives the dose time to fully deposit into subcutaneous tissue. Withdraw smoothly, dispose of the needle in a sharps container (never a regular bin), and apply gentle pressure to the site with a cotton pad if needed. Do not rub.
A simple 4-week semaglutide rotation schedule
| Week | Site |
|---|---|
| Week 1 | Right side of abdomen |
| Week 2 | Left thigh, front |
| Week 3 | Left side of abdomen |
| Week 4 | Right thigh, front |
If you have a helper, you can swap one of the abdomen weeks for an upper-arm injection.
Want to start a course? Browse generic semaglutide and other GLP-1 options at MedsBase — no prescription needed, Worldwide Shipping, every order covered by our Reshipment Assurance policy.
Frequently Asked Questions
Where is the best place to inject semaglutide?
There is no single “best” site — the abdomen, front of thigh and back of upper arm are all approved and clinically equivalent. Most users choose the abdomen because it’s the easiest to see and reach for self-injection. The most important factor is rotating between sites to prevent skin and tissue changes over time.
Does it matter where you inject Ozempic?
For absorption, no — published pharmacokinetic data shows semaglutide is bioequivalent across all three approved sites. What does matter is consistency in technique, using a new needle each time, and rotating between sites. Choose the site that’s most comfortable for you and works with your weekly schedule.
Can I inject semaglutide in my arm by myself?
Technically yes, but it’s awkward for most people because the back of your upper arm is hard to reach with your own hand. Self-injecting in the arm often results in a poor needle angle or a missed pinch. If the arm is your preferred site, asking a partner or family member to help is more practical than struggling alone.
Why do you have to rotate semaglutide injection sites?
Repeated injections into exactly the same spot can cause lipohypertrophy — small lumps of thickened fatty tissue that may also reduce future absorption from that area. Rotation gives each site time to heal between doses. The principle was first established in insulin literature decades ago and applies equally to GLP-1 drugs.
Does injecting semaglutide in the stomach work faster?
No. Although abdominal injection is sometimes thought to absorb faster, this only applies to fast-acting medicines like mealtime insulin. Semaglutide has a one-week half-life and is designed for slow, steady release — site choice doesn’t change how quickly it reaches a useful blood concentration.
Is it less painful to inject semaglutide in the thigh?
Pain perception is highly individual. Many users find the thigh slightly more uncomfortable for the first hour after injection because walking puts pressure on the area. Others find the abdomen more sensitive after meals. The biggest pain-reducer is technique: a fresh needle, a 90° insertion angle and letting the alcohol swab fully dry.
How long do I have to hold the needle in after pressing the button?
At least 6 seconds. This gives the dose time to fully deposit into subcutaneous tissue before you withdraw. Pulling the needle out too quickly is one of the most common causes of a “leaky” injection — where some of the dose ends up on the skin instead of in the body.
Can I inject semaglutide through clothing?
No. Even thin fabric can carry skin bacteria into the injection site, dulls the needle and prevents you from properly inspecting the skin. Always inject directly into clean, exposed skin that has been wiped with an alcohol swab.
The bottom line
The three approved semaglutide injection sites — abdomen, front of thigh and back of upper arm — are clinically equivalent. Your dose will work the same whichever zone you choose. What actually moves the needle on comfort, consistency and long-term skin health is two simple habits: use a fresh needle every time and rotate sites week to week.
If you’re starting a course, the abdomen is the easiest first choice for most users — but adopt a rotation pattern from week 1, not from when irritation appears. A four-site rotation across abdomen-left, abdomen-right, thigh-left and thigh-right keeps every zone well-rested between doses.
For users sourcing semaglutide for chronic weight management or type 2 diabetes, MedsBase carries WHO-GMP certified generic semaglutide alongside research-grade options in the peptides catalogue. Every order is covered by our Reshipment Assurance policy and shipped with Worldwide Shipping — no prescription needed.
Medical Disclaimer
This article is for general educational purposes only and is not a substitute for personalised medical advice. Semaglutide is a potent medication with significant effects on blood sugar, appetite and gastrointestinal function. Always consult a qualified healthcare professional before starting, stopping or adjusting any GLP-1 medication, and seek immediate care for any signs of allergic reaction, severe abdominal pain, vision changes or unusual symptoms. Information here reflects published evidence and product labelling at the time of last review (15 May 2026) and may change as new data emerges.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.