







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

In May 2022, the FDA approved tirzepatide for type 2 diabetes. Within 24 months, it had become the most-talked-about weight-loss medication in the world — and the first incretin-based drug to deliver weight loss approaching what previously required bariatric surgery. Semaglutide, the molecule that launched the modern GLP-1 era, suddenly had a rival.
If you’re choosing between tirzepatide vs semaglutide — or trying to understand whether it’s worth switching — this guide walks through exactly how they differ. You’ll see the head-to-head clinical data, how the mechanisms actually diverge at the cellular level, how dosing and side effects compare, what the typical cost difference looks like, and who tends to benefit more from each.
- Tirzepatide activates two gut-hormone receptors (GIP and GLP-1); semaglutide activates only one (GLP-1).
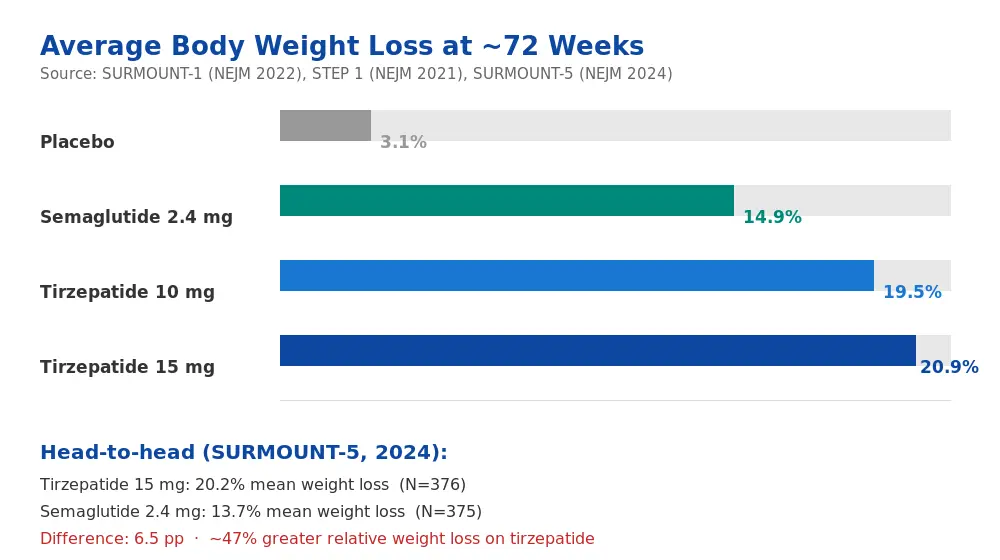
- In the head-to-head SURMOUNT-5 trial (NEJM 2024), tirzepatide produced ~47% greater relative weight loss than semaglutide over 72 weeks.
- Side-effect profiles are similar, dominated by gastrointestinal symptoms — tolerability differences are modest.
- Semaglutide has the only confirmed cardiovascular-outcomes trial win (SELECT, 2023); tirzepatide’s CV data is expected in 2027.
- Cost, availability, and prescriber preference often decide real-world choice more than efficacy differences.
What Is Tirzepatide and What Is Semaglutide?
Tirzepatide and semaglutide are both once-weekly injectable medications developed to treat type 2 diabetes, later approved for chronic weight management. They belong to a broader drug class called incretin mimetics — synthetic molecules that copy the action of gut hormones our bodies release after eating.
Semaglutide was approved by the FDA for type 2 diabetes in 2017 (as Ozempic) and for chronic weight management in 2021 (as Wegovy, at a higher dose). It acts on a single receptor: GLP-1 (glucagon-like peptide-1). Rybelsus, the oral tablet form, came in 2019 — currently the only oral drug in the class.
Tirzepatide was approved for type 2 diabetes in 2022 (as Mounjaro) and for chronic weight management in late 2023 (as Zepbound). It is the first dual agonist in clinical use — it binds to and activates both the GLP-1 receptor and the GIP (glucose-dependent insulinotropic polypeptide) receptor.
That single structural difference — one receptor versus two — is responsible for most of the clinically meaningful differences you’ll see in this article.
How Does Each Drug Work? The Mechanism Difference That Changes Everything
Both drugs borrow from the body’s natural incretin system — the hormones GLP-1 and GIP that the small intestine releases after a meal. These hormones:
- Signal the pancreas to release insulin (but only when blood glucose is elevated)
- Slow gastric emptying so food moves through the stomach more slowly
- Suppress glucagon (a hormone that raises blood sugar)
- Act on appetite centres in the brain to reduce hunger and food intake
Semaglutide’s mechanism: it is a synthetic analogue of GLP-1, modified so it resists rapid breakdown by the enzyme DPP-4. This lets it remain active in the bloodstream for about a week. It binds to the GLP-1 receptor and produces all of the effects above — but only via that single pathway.
Tirzepatide’s mechanism: it is a single molecule that activates both the GLP-1 and the GIP receptors. GIP’s role in appetite and metabolism was underappreciated for decades — older research suggested it was neutral or even slightly obesogenic. More recent work has shown that when paired with GLP-1 activation, GIP amplifies insulin secretion, improves insulin sensitivity in peripheral tissues, and adds an independent appetite-regulating signal.
That is the molecular reason tirzepatide produces, on average, larger effects than semaglutide. It isn’t a stronger dose of the same drug — it’s a different drug with a broader signalling footprint.
Key Uses and Who Each Drug Is For
Both medications are approved for two overlapping conditions: type 2 diabetes and chronic weight management. But their real-world fit varies.
Type 2 Diabetes Management
Both drugs produce meaningful reductions in HbA1c and fasting glucose. In the SURPASS-2 trial (tirzepatide vs semaglutide 1 mg head-to-head in type 2 diabetes), tirzepatide produced a 1.9–2.1% HbA1c reduction at the higher doses versus about 1.5% for semaglutide at 1 mg. Both dramatically outperform older drug classes like sulfonylureas and DPP-4 inhibitors.
Chronic Weight Management
Chronic weight management is where the two drugs diverge most visibly.
- Semaglutide 2.4 mg (Wegovy) produces average weight loss of 14.9% of body weight over 68 weeks in non-diabetic adults with obesity (STEP 1 trial).
- Tirzepatide 15 mg (Zepbound) produces average weight loss of 20.9% of body weight over 72 weeks in the same population (SURMOUNT-1 trial).
Cardiovascular Risk Reduction
This is currently the one area where semaglutide has a clear evidence advantage. The SELECT trial (2023) showed semaglutide reduced major adverse cardiovascular events by 20% in adults with overweight or obesity and established cardiovascular disease. Tirzepatide’s cardiovascular outcomes trial (SURPASS-CVOT) is still ongoing, with topline data expected in 2027.
Other Emerging Uses
Both drugs are being studied for obstructive sleep apnoea, metabolic dysfunction-associated steatohepatitis (MASH), heart-failure with preserved ejection fraction (HFpEF), chronic kidney disease, and some neurodegenerative conditions. Tirzepatide received FDA approval for moderate-to-severe obstructive sleep apnoea with obesity in December 2024.
Safety Profile, Side Effects, and Tolerability
Side-Effect Frequency (Pooled Trial Data)
| Side effect | Tirzepatide 15 mg | Semaglutide 2.4 mg | Severity (most cases) |
|---|---|---|---|
| Nausea | 29% | 44% | Mild–moderate, improves with titration |
| Diarrhoea | 23% | 30% | Mild |
| Vomiting | 13% | 24% | Mild–moderate |
| Constipation | 12% | 24% | Mild |
| Abdominal pain | 10% | 20% | Mild |
| Injection-site reaction | 5% | 8% | Mild |
| Hypoglycaemia (non-diabetic) | <1% | <1% | Rare |
| Acute pancreatitis | <0.2% | <0.2% | Rare, reported in both |
Data pooled from SURMOUNT-1 (Jastreboff et al., NEJM 2022) and STEP 1 (Wilding et al., NEJM 2021). In the direct head-to-head SURMOUNT-5 trial (2024), discontinuation rates due to adverse events were similar between groups — about 6% on tirzepatide and 8% on semaglutide.
Serious Warnings (Both Drugs)
- Medullary thyroid carcinoma (MTC): Both carry a boxed warning based on rodent studies. Neither should be used in patients with a personal or family history of MTC or multiple endocrine neoplasia type 2 (MEN 2).
- Pancreatitis: Rare but reported with both; patients with a history of pancreatitis are generally excluded.
- Gallbladder disease: Rapid weight loss increases gallstone risk; both drugs have elevated rates of cholelithiasis versus placebo.
- Gastroparesis: Both slow gastric emptying significantly; caution in patients with pre-existing gastroparesis.
What Does the Research Say?
The evidence base on both drugs is now extensive. Here is a summary of the landmark and head-to-head trials.
| Study | Year | Drug(s) | Key finding |
|---|---|---|---|
| STEP 1 | 2021 | Semaglutide 2.4 mg vs placebo | 14.9% mean weight loss at 68 wks |
| SURMOUNT-1 | 2022 | Tirzepatide 5/10/15 mg vs placebo | 15%, 19.5%, 20.9% weight loss at 72 wks |
| SURPASS-2 | 2021 | Tirzepatide vs semaglutide 1 mg (T2D) | Tirzepatide superior on HbA1c and weight |
| SELECT | 2023 | Semaglutide 2.4 mg vs placebo (CV outcomes) | 20% reduction in major adverse CV events |
| SURMOUNT-5 | 2024 | Tirzepatide vs semaglutide (head-to-head) | Tirzepatide 20.2% vs semaglutide 13.7% at 72 wks |
| SURPASS-CVOT | ongoing | Tirzepatide vs dulaglutide (CV outcomes) | Results expected 2027 |
SURMOUNT-5 deserves particular attention. It is the first and only head-to-head randomised trial of tirzepatide vs semaglutide for weight loss in adults with obesity (without type 2 diabetes). Published in The New England Journal of Medicine in 2024, it found tirzepatide produced roughly 47% greater relative weight loss than semaglutide at equivalent trial endpoints, with broadly comparable tolerability.
Research suggests — though long-term data are still accumulating — that the efficacy advantage of tirzepatide persists at 2+ years of continuous treatment.
Tirzepatide vs Semaglutide — Direct Comparison Table
| Criterion | Tirzepatide | Semaglutide |
|---|---|---|
| Mechanism | Dual GIP + GLP-1 agonist | GLP-1 agonist only |
| Weekly injectable brands | Mounjaro (T2D), Zepbound (obesity) | Ozempic (T2D), Wegovy (obesity) |
| Oral formulation | No | Yes (Rybelsus, T2D only) |
| Dosing frequency | Once weekly | Once weekly (inj); daily (oral) |
| Maximum dose | 15 mg weekly | 2.4 mg (obesity); 2.0 mg (T2D) |
| Avg weight loss (~72 wks, obesity) | 20–21% | 14–15% |
| HbA1c reduction (T2D, max dose) | 2.0–2.1% | 1.5–1.8% |
| Cardiovascular outcomes data | Pending (2027) | Confirmed (SELECT, 2023) |
| FDA approval (obesity) | Nov 2023 | Jun 2021 |
| Typical monthly cost (US list) | ~$1,000–1,200 | ~$1,000–1,350 |
| GI side-effect frequency | Slightly lower at equivalent weight loss | Slightly higher at equivalent weight loss |
How to Use Each Drug Safely
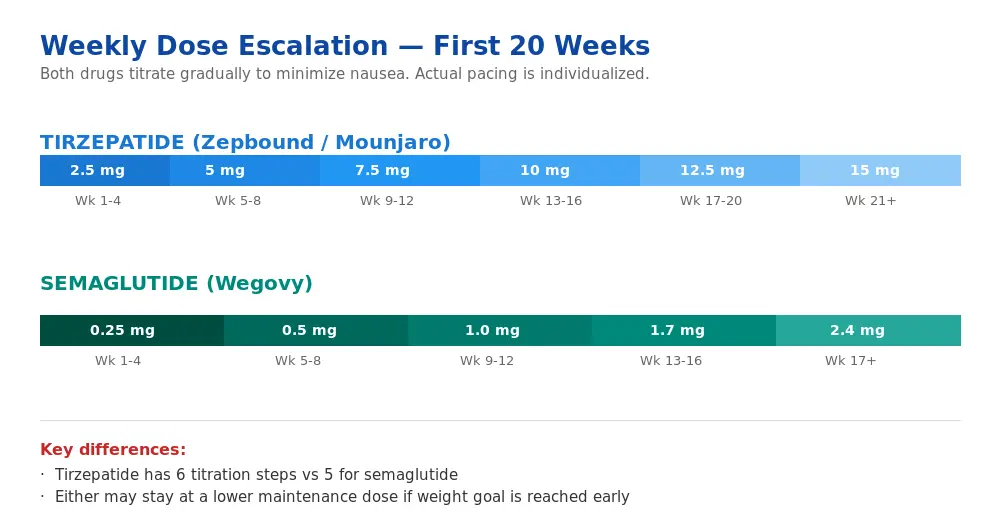
Both drugs require a slow dose-escalation schedule. Starting at the maximum dose — or titrating too quickly — is the single most common reason for severe nausea, vomiting, and treatment discontinuation.
Semaglutide (Wegovy, Weight Management)
- Weeks 1–4: 0.25 mg once weekly
- Weeks 5–8: 0.5 mg once weekly
- Weeks 9–12: 1.0 mg once weekly
- Weeks 13–16: 1.7 mg once weekly
- Week 17 onward: 2.4 mg once weekly (maintenance)
Tirzepatide (Zepbound, Weight Management)
- Weeks 1–4: 2.5 mg once weekly
- Weeks 5–8: 5 mg once weekly
- Weeks 9–12: 7.5 mg (or stay at 5 mg if tolerating well)
- Weeks 13–16: 10 mg
- Weeks 17–20: 12.5 mg (optional)
- Week 21 onward: 15 mg (maximum)
If tolerability is a challenge at any step, clinicians typically extend that dose for an additional 4 weeks before advancing. Maintenance doses are highly individual — many patients achieve goal weight on 7.5 or 10 mg tirzepatide and never need 15 mg.
Practical Guidance (Both Drugs)
- Inject into the abdomen, thigh, or upper arm; rotate sites weekly
- Store pens refrigerated before first use; after first use, most can be kept at room temperature for 21–42 days depending on the product
- Take your injection on the same day each week; you can shift by up to 48 hours if needed
- Don’t double-dose after a missed dose — skip and resume on schedule
- Avoid alcohol during rapid titration; it amplifies nausea
Browse MedsBase’s men’s health and weight-management catalogue or our peptides range for discreet worldwide shipping on both molecules in multiple strengths.
Cost Comparison
In 2026, unsubsidised list prices in the US remain broadly similar — roughly $1,000–$1,350/month for branded semaglutide (Wegovy or Ozempic) and $1,000–$1,200/month for branded tirzepatide (Zepbound or Mounjaro) at maximum dose.
The real-world cost picture, however, depends heavily on:
- Insurance coverage: coverage for obesity indications has expanded in 2025–2026 but remains inconsistent; diabetes indications are broadly covered
- Country: the same molecule can cost 60–80% less outside the US, particularly for globally-sourced generics
- Compounded availability: compounded versions exist where the branded drug is in shortage (status varies by country and regulatory jurisdiction)
- Savings programmes: manufacturers offer patient-assistance cards that can reduce out-of-pocket by hundreds per month in the US
For most international patients, the practical cost difference between tirzepatide and semaglutide is small — the choice comes down to efficacy, tolerability, and prescriber preference, not price.
Can You Switch From Semaglutide to Tirzepatide (or Vice Versa)?
Yes, and this is increasingly common. Because the two drugs share the GLP-1 pathway, switching usually doesn’t require a washout period — your last semaglutide dose can be followed seven days later by a starting dose of tirzepatide.
The starting dose on the new drug, however, should be low regardless of where you were on the old one. Jumping from semaglutide 2.4 mg directly to tirzepatide 15 mg is almost guaranteed to trigger severe nausea. Standard clinical practice is to restart tirzepatide at 2.5–5 mg and re-titrate, which most patients tolerate well because their gastric-emptying adaptation from semaglutide carries over partially.
Reasons people switch:
- Plateau on semaglutide (weight loss stalled)
- Intolerable side effects on one drug that don’t replicate on the other
- Supply / availability shifts
- Cost differences in local markets
Reasons people stay on semaglutide despite tirzepatide’s higher efficacy:
- Confirmed cardiovascular-event reduction (SELECT)
- Oral option (Rybelsus) for needle-averse patients with T2D
- Longer post-marketing safety experience
- Established coverage under their insurance plan
Frequently Asked Questions
Is tirzepatide stronger than semaglutide?
On average, yes — but “stronger” is a loaded term. Tirzepatide produces greater weight loss and greater HbA1c reduction in head-to-head trials, largely because it acts on two gut-hormone receptors instead of one. However, “stronger” also means a slightly higher incidence of GI side effects in some patients and less long-term safety data. The right choice depends on goals, tolerance, and co-existing conditions.
How much more weight do people lose on tirzepatide vs semaglutide?
In the SURMOUNT-5 head-to-head trial, tirzepatide produced about 20.2% mean body-weight loss at 72 weeks vs 13.7% for semaglutide — roughly a 6.5 percentage-point absolute difference, or about 47% more weight lost on tirzepatide in relative terms. Individual results vary significantly.
Which has worse side effects, tirzepatide or semaglutide?
Both drugs produce similar categories of side effects — mostly gastrointestinal. Pooled trial data suggest semaglutide reports slightly more nausea and vomiting at maximum dose, while tirzepatide at its highest dose reports slightly higher GI symptom frequency than tirzepatide at mid-dose. Discontinuation rates due to side effects are similar (about 6–8%) between the two drugs.
Can you switch from Ozempic to Mounjaro?
Yes. Most clinicians initiate tirzepatide at its starting dose of 2.5 mg weekly, one week after the final semaglutide dose, then re-titrate. Don’t attempt a direct dose-for-dose conversion — the two drugs aren’t equipotent and starting high causes severe nausea.
Is there a generic tirzepatide or semaglutide?
No FDA-approved generic exists for either molecule as of 2026 — both remain under patent. However, globally-sourced and compounded versions are available through various regulated international channels and during US/EU shortage periods. Quality and sourcing vary; always verify your pharmacy’s credentials.
Do I have to stay on it forever?
Not necessarily “forever,” but both drugs are designed for chronic use, and stopping either typically leads to partial weight regain over 12 months (STEP 4 and SURMOUNT-4 trials). Think of them more like medications for hypertension or asthma — effective while taken, less effective when discontinued. Long-term strategies usually involve staying on a maintenance dose or tapering carefully with intensive lifestyle support.
Which is better for type 2 diabetes specifically?
Tirzepatide produces greater HbA1c reductions head-to-head (SURPASS-2), but semaglutide has the stronger cardiovascular-outcomes evidence (SELECT, SUSTAIN-6). For patients with established cardiovascular disease, many clinicians still favour semaglutide. For patients prioritising glucose and weight, tirzepatide has the edge. The SURPASS-CVOT trial results in 2027 may narrow this gap.
Can I take tirzepatide and semaglutide together?
No. Combining two GLP-1 receptor agonists is not recommended — there is no evidence of added benefit, and side effects (especially GI and hypoglycaemia risk in T2D) compound significantly. If one drug isn’t working adequately, the standard approach is to switch, not stack.
The Bottom Line
Tirzepatide and semaglutide are both remarkable drugs — medications that have genuinely shifted what’s possible in obesity and type 2 diabetes care. The honest verdict, based on the 2026 evidence base:
- For maximum weight loss, tirzepatide has a real and measurable advantage (~5–7 percentage points of body-weight loss in head-to-head data).
- For confirmed cardiovascular risk reduction in high-risk patients, semaglutide remains the only drug in the class with outcome-trial wins.
- For tolerability, they are broadly similar — individual response varies more than the average difference.
- For cost and access, the choice often comes down to local supply and insurance, not drug pricing.
Neither drug is universally “better.” The right answer depends on what you’re optimising for, your other health conditions, your tolerance of injections and GI side effects, and what your prescriber recommends based on your specific history.
The real story is that, in 2026, patients have two genuinely effective options for a condition that for decades had almost none. That is the breakthrough — not the race between them.
Browse MedsBase’s full men’s health and weight-management range, our peptide therapy catalogue, or see our credit card and cryptocurrency payment guides for medically-sourced options with discreet worldwide shipping.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.