







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
By age 50, roughly half of men and a quarter of women notice visible hair loss. It is one of the most common cosmetic concerns in medicine — and one of the most misunderstood. Behind every claim of a “miracle supplement,” “hair regrowth laser,” or “natural DHT blocker” sits a small handful of treatments that actually work and a clear clinical playbook for using them.
This is a complete, evidence-based hair loss treatment guide for 2026. It covers what hair loss actually is, the different types (and why diagnosing yours matters more than any product choice), how the Norwood scale stages progression in men, which medications genuinely regrow hair, how long to wait before judging results, when surgery becomes the right option, and what lifestyle factors amplify every other treatment you try. Written for men and women, with evidence-based recommendations for both.
- Androgenetic alopecia — male and female pattern hair loss — accounts for 95% of all hair loss cases and is driven by DHT.
- Only three medical treatments have strong evidence: minoxidil (topical or oral), finasteride, and dutasteride.
- Combination therapy (finasteride + minoxidil) is the most effective non-surgical approach — around 94% see stabilisation or regrowth at 12 months.
- Starting early matters. Treatment preserves existing hair. It cannot revive follicles that have fully died.
- Temporary hair loss (telogen effluvium) resolves on its own in 3-6 months — don’t over-treat it.
- Hair transplant surgery (FUE or FUT) is the only option for late-stage pattern hair loss but is cosmetic, not curative.
What Is Hair Loss?
Quick Answer: What counts as hair loss?
Shedding 50-100 hairs per day is normal. Hair loss is meaningful when you notice a persistent increase in shedding, visible thinning at the crown or temples, a widening part, or circular bald patches. Any of those lasting more than 3 months justifies a dermatology review — most causes are treatable, but early intervention produces better results than delayed treatment.
Hair follows a four-phase growth cycle. Anagen (active growth) lasts 2-7 years and produces roughly 90% of scalp hair at any given time. Catagen (transition) lasts 2-3 weeks. Telogen (rest) lasts 3-4 months. Exogen (shedding) releases the dormant hair so a new one can start.
Hair loss occurs when this cycle is disrupted. Hairs may shed prematurely (telogen effluvium), fail to regrow at all (androgenetic alopecia or scarring alopecia), or be attacked by the immune system (alopecia areata). The pattern and timing of loss is the single most important clue to which cause is driving it — and therefore which treatment will actually work.
The American Academy of Dermatology estimates that more than 80 million Americans have some form of hair loss. Globally, androgenetic alopecia affects about 50% of men over 50 and 40% of women over 50. The proportion has been rising slowly, likely due to a combination of delayed diagnosis, dietary factors, and increased awareness pushing more people to formal clinical measurement.
Types of Hair Loss — Getting the Diagnosis Right
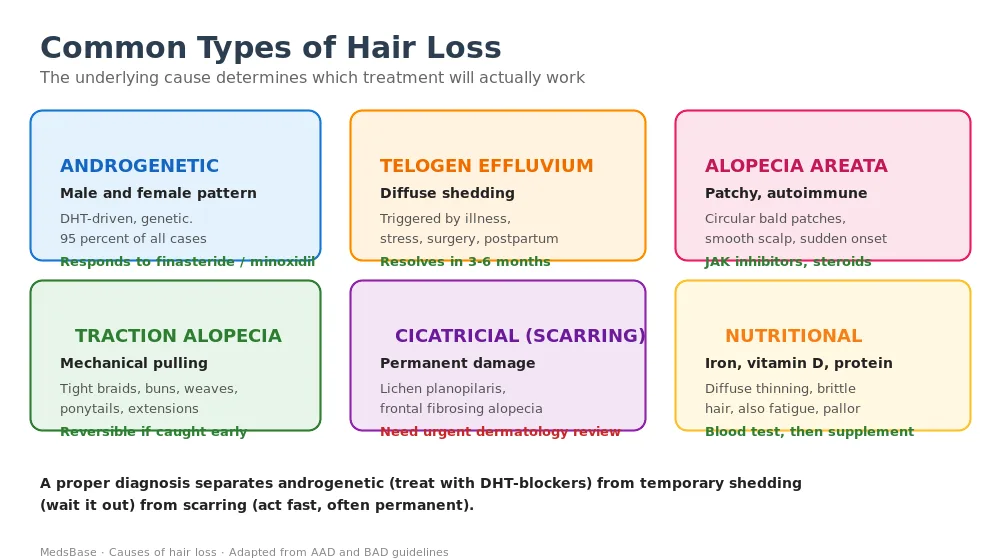
Androgenetic alopecia (male / female pattern)
By far the most common. A genetically inherited sensitivity to dihydrotestosterone (DHT) causes progressive follicle miniaturisation, producing thinner, shorter, less pigmented hairs until finally the follicle stops producing terminal hair altogether. In men it follows the Norwood pattern (receding temples, crown thinning). In women it follows the Ludwig pattern (diffuse thinning across the crown with intact frontal hairline). Responds well to minoxidil and (in men) finasteride/dutasteride.
Telogen effluvium
Diffuse shedding from across the scalp, typically starting 2-3 months after a trigger: major illness, surgery, childbirth, severe weight loss, thyroid disorder, starting or stopping certain medications, or extreme stress. Hair count can drop dramatically for 3-6 months before recovering on its own. Reassurance and patience is the treatment — most cases fully resolve without medication.
Alopecia areata
Autoimmune attack on hair follicles, producing smooth circular bald patches that appear suddenly — often on the scalp but sometimes on the beard, eyebrows, or elsewhere. About half of cases resolve spontaneously. Severe cases (alopecia totalis, alopecia universalis) now have a genuinely effective treatment in the JAK inhibitors (baricitinib, ritlecitinib) approved since 2022.
Traction alopecia
Caused by sustained mechanical pulling — tight braids, weaves, high ponytails, extensions, dreadlocks, certain religious headwear, or aggressive brushing. Affects the frontal and temporal hairline first. Entirely preventable, and fully reversible if the offending style is abandoned within 1-2 years. After that, scarring develops and loss becomes permanent.
Cicatricial (scarring) alopecia
A group of rarer conditions — lichen planopilaris, central centrifugal cicatricial alopecia (CCCA), frontal fibrosing alopecia, folliculitis decalvans — where inflammation destroys the follicle and replaces it with scar tissue. Requires urgent dermatology review because once scarring happens, hair cannot return. Treatment aims to halt progression with topical steroids, oral immunosuppressants, or hydroxychloroquine depending on subtype.
Nutritional / endocrine hair loss
Iron deficiency (especially in menstruating women), vitamin D deficiency, zinc deficiency, severe protein restriction (crash diets, bariatric surgery), or thyroid dysfunction all cause diffuse thinning. Blood testing uncovers the cause and replacement reverses the loss within 6 months.
The Norwood-Hamilton Scale — Staging Male Pattern Hair Loss
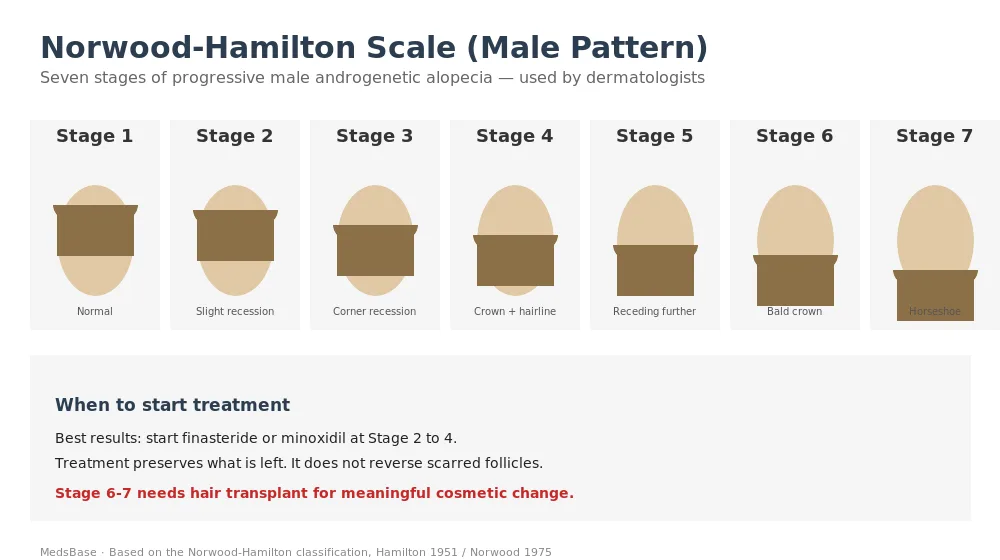
The Norwood-Hamilton scale (originally devised by Hamilton in 1951, modified by Norwood in 1975) is the universal reference for staging male pattern hair loss.
Stages 1-2 are essentially normal or very mild — slight recession at the temples that most men have by their 30s. No treatment needed.
Stages 3-4 represent the window where pharmacological treatment produces the biggest gains. Finasteride or minoxidil started now can preserve most existing hair indefinitely and generate meaningful regrowth in half to two-thirds of men.
Stages 5-7 represent advanced loss. Medication can still halt progression, but the follicles already lost cannot be restored by drugs. Hair transplantation becomes the only option for visible cosmetic improvement.
The practical rule: take two good photos of your hairline and crown annually, in the same lighting. Comparing year-over-year reveals progression long before the mirror does.
Why Does Hair Loss Happen? The DHT Pathway
For the 95% of cases driven by androgenetic alopecia, the mechanism is well understood. Testosterone is converted by the enzyme 5-alpha-reductase into dihydrotestosterone (DHT) — a more potent androgen. Men and women both produce DHT in varying quantities.
In genetically susceptible follicles, DHT binds to androgen receptors on the hair papilla and triggers progressive miniaturisation. Each growth cycle produces a thinner, shorter, less pigmented hair. Over 5-15 years, terminal hair is replaced by vellus hair (fine “peach fuzz”) — and eventually the follicle stops producing hair at all.
Two implications follow:
- Blocking DHT production (with finasteride or dutasteride) slows or halts the process. For detailed head-to-head data, see our finasteride vs dutasteride comparison.
- Stimulating follicle activity (with minoxidil) extends the anagen growth phase and prolongs the useful life of each follicle. See our minoxidil 5% vs 10% guide for strength-specific data.
The two mechanisms are complementary, which is why combination therapy outperforms either drug alone.
How Hair Loss Is Diagnosed
A good dermatologist relies mostly on history and examination. A standard workup includes:
- Detailed history — onset, pattern, family history, medications, pregnancies, crash diets, thyroid symptoms, stress events.
- Scalp examination under dermatoscopy — reveals follicular miniaturisation, peripilar signs, broken hairs, or scarring.
- Pull test — gently pulling a small tuft. More than 6 hairs released suggests active shedding.
- Blood work — ferritin (aim above 50), vitamin D, TSH, zinc, and for women experiencing sudden hair loss, a hormonal panel (free/total testosterone, DHEA-S, prolactin).
- Scalp biopsy — reserved for suspected scarring alopecia or unclear cases.
Most diagnoses can be confirmed in a 15-minute consultation by a dermatologist familiar with hair loss. A “trichologist” is not a medical doctor and cannot prescribe treatment.
Treatment Options — What Actually Works
Minoxidil (topical or oral)
Originally developed as a blood-pressure drug, minoxidil causes vasodilation in the scalp and extends the anagen (growth) phase of the hair cycle. Available as:
- Topical 2% solution — for women, applied twice daily.
- Topical 5% solution or foam — the standard for men; often used for women with stubborn cases. The foam is alcohol-free and better tolerated on sensitive scalps.
- Topical 10% compounded solution — stronger but not significantly more effective than 5%; higher irritation rate.
- Oral minoxidil 2.5-5 mg daily — off-label but increasingly popular. Bypasses topical-application fatigue; slightly higher response rate; minor side effects (facial hair growth, ankle swelling in some).
Expect 4-6 months before visible effect. Continued use is required — stopping returns hair density to pre-treatment baseline within 3-6 months.
Finasteride (oral, 1 mg daily)
Blocks type-II 5-alpha-reductase, reducing scalp DHT by around 60%. FDA-approved for male pattern hair loss since 1997. Response rate of 86% at 1 year (stabilisation or regrowth). Side effects — reduced libido, erectile dysfunction, breast tenderness — affect about 2-4% of users. Most reverse on stopping; a minority report persistent symptoms (post-finasteride syndrome). Not used in women of reproductive age due to severe teratogenic risk.
Dutasteride (oral, 0.5 mg daily)
Blocks both type-I and type-II 5-alpha-reductase, reducing scalp DHT by around 79%. Off-label for hair loss in most countries (FDA-approved in South Korea and Japan). About 20% more effective than finasteride at 12 months in head-to-head data. Slower washout — half-life around 5 weeks — which matters for family-planning considerations. Browse Proscalpin (generic finasteride) and related oral options in our catalogue.
Combination therapy
Finasteride + minoxidil together produces the best non-surgical outcome. In clinical studies, about 94% of men see stabilisation or regrowth at 12 months with the combination. The two drugs have independent mechanisms, so adding one to the other produces genuine incremental effect — not just tolerance-stacking.
Platelet-rich plasma (PRP) and microneedling
Both stimulate follicle activity through growth-factor signalling and mild wounding. Evidence is modest but positive — around 50% of men see some improvement when added to standard therapy. Treatment involves monthly sessions for 3-6 months, then maintenance every 3-6 months. Cost is significant and insurance rarely covers it. Not a substitute for medical therapy.
Low-level laser therapy (LLLT)
Red-light helmets and combs emit 650-nanometre light that may stimulate mitochondrial activity in the hair bulb. Evidence is modest but positive for AGA. Convenient, safe, and can be used at home. Usually an adjunct rather than standalone.
Hair transplant surgery (FUE and FUT)
The only true reversal for advanced pattern hair loss. FUE (follicular unit extraction) harvests individual grafts from the donor area — labour-intensive but leaves no linear scar. FUT (follicular unit transplantation) removes a strip of scalp and dissects it into grafts under microscope — faster and cheaper per graft but leaves a linear scar. Both require ongoing medical therapy afterwards, because the un-transplanted native hair continues to miniaturise without treatment.
JAK inhibitors (for alopecia areata only)
A genuinely transformative option approved since 2022 for severe alopecia areata. Baricitinib and ritlecitinib produce substantial regrowth in 30-40% of users with alopecia totalis or universalis. Not effective for androgenetic alopecia.
Efficacy Compared — Head-to-Head Data
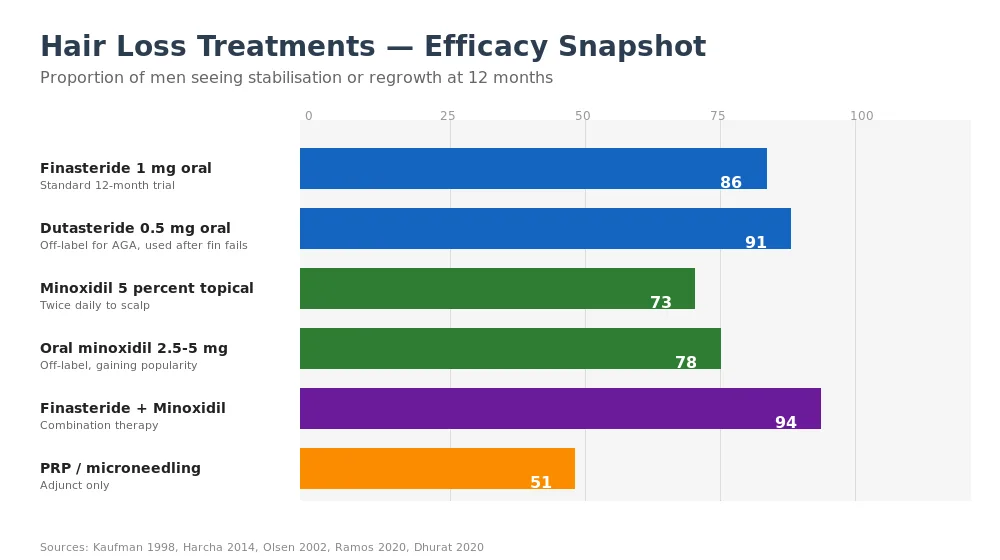
Research suggests — consistently across more than 30 randomised trials since 1998 — that:
- Finasteride monotherapy stabilises or regrows hair in ~86% of men at 12 months.
- Dutasteride monotherapy produces ~91% response — slightly higher than finasteride in head-to-head trials.
- Topical minoxidil 5% produces ~73% response.
- Oral minoxidil 2.5-5 mg produces ~78% response — slightly higher than topical, with better adherence.
- Finasteride + minoxidil combination produces ~94% response — the gold standard.
- PRP as adjunct adds 10-15 percentage points to the baseline combination response.
The best single-pill choice today is finasteride (or dutasteride if finasteride fails). The best topical is minoxidil 5% foam. The best evidence-based regimen for serious hair loss is combination therapy plus scalp-health basics.
Realistic Regrowth Timeline — What to Actually Expect

Months 0-3: the dread shed. Both finasteride and minoxidil push dormant-cycle hairs out of the scalp to make room for new growth. Shedding increases, sometimes dramatically. This is paradoxically a sign the treatment is working, but it is the phase in which most men quit.
Months 3-6: stabilisation. Shedding slows. Early signs of finer regrowth at the hairline and crown become visible under good lighting. Measured hair count starts rising.
Months 6-12: visible regrowth. This is when annual photos finally reveal the payoff — density increases, miniaturised areas begin producing terminal hair again. Most men see their peak regrowth between month 9 and month 15.
Month 12+: maintenance. Gains plateau. Continued treatment preserves what you’ve built; stopping returns hair to pre-treatment baseline within 9-12 months. This is a lifelong commitment. Treating androgenetic alopecia is less like an antibiotic course and more like managing high blood pressure.
Female Pattern Hair Loss — Similar Disease, Different Playbook
Women can experience androgenetic hair loss too, though the pattern differs. Where men recede at temples and crown, women typically thin diffusely across the top of the scalp with an intact frontal hairline — the Ludwig pattern.
First-line treatment for women is minoxidil (2% twice daily or 5% once daily foam). Response rates are slightly lower than in men — around 60% see meaningful improvement. Finasteride is not first-line in women because of teratogenic risk and mixed efficacy data in pre-menopausal women.
Other options specific to women:
- Low-dose oral minoxidil (0.25-1 mg daily) — emerging off-label favourite for women, with excellent tolerability and effect comparable to topical.
- Spironolactone (50-200 mg daily) — an aldosterone antagonist with anti-androgen properties. Effective in women with hormone-driven hair loss, particularly PCOS.
- Oral contraceptive pills containing anti-androgenic progestins (drospirenone, cyproterone acetate) — can help when PCOS drives hair loss.
- Dutasteride off-label — used in post-menopausal women with careful counselling.
For broader context, see our dedicated guide on treating androgenic hair loss in women.
Lifestyle Habits That Protect Your Hair

Adequate protein (around 1.2 g per kg body weight)
Hair is 90% keratin. Protein-restricted diets — aggressive cutting, veganism without planning, post-bariatric — often present as diffuse hair loss within 2-3 months. The fix is straightforward: more protein.
Iron and ferritin above 50 ng/mL
Iron deficiency is the single most common reversible cause in menstruating women. Ferritin below 30 is typically linked to active shedding even in the absence of overt anaemia. Supplement guided by blood work, not guesswork.
Vitamin D 30-50 ng/mL
Low vitamin D is associated with both androgenetic alopecia and alopecia areata. Supplementation is cheap, safe, and removes one variable.
Quit smoking
Smokers develop pattern hair loss faster than non-smoking siblings in twin studies. Nicotine constricts scalp vessels and accelerates oxidative damage to follicles. Quitting slows the trajectory.
Manage chronic stress
Chronic elevated cortisol disrupts the hair cycle and is a leading trigger of telogen effluvium. Regular exercise, adequate sleep, and mindfulness practice all reduce cortisol load. Hair responds over 6-12 months.
Gentle hair care
Avoid tight ponytails, buns, braids, and extensions. Use low-heat tools. Don’t over-wash or over-dry. These habits won’t regrow hair but they stop unnecessary additional loss.
See also our in-depth guides: Can you prevent hair loss before it’s too late?, How to stop hair loss, and 6 foods that may block DHT.
Frequently Asked Questions
Is hair loss reversible?
It depends on the cause. Telogen effluvium, iron-deficiency hair loss, and traction alopecia (caught early) are fully reversible. Androgenetic alopecia is controllable but not curable — treatment preserves existing follicles and encourages regrowth, but requires ongoing use. Scarring alopecia is largely irreversible once scarring has occurred. Early diagnosis is the strongest predictor of a good outcome.
At what age does hair loss start?
Androgenetic hair loss can begin any time after puberty but most commonly starts between 20 and 40 in men, and around perimenopause in women. Starting treatment earlier — while follicles are still producing terminal hair — produces markedly better results than waiting until loss is visible.
Does stress really cause hair loss?
Yes, through a mechanism called telogen effluvium. Major physical or emotional stress pushes follicles prematurely into the resting phase; shedding appears 2-3 months later. The trigger might be surgery, severe illness, bereavement, divorce, financial shock, or acute infection (including COVID-19, which produced a measurable global wave of telogen effluvium in 2020-2021). Most cases resolve in 3-6 months without any treatment.
Which vitamin deficiency causes hair loss?
Iron, vitamin D, zinc, biotin, and vitamin B12 have all been linked to hair loss when severely deficient. The most common in practice is iron (especially in menstruating women). Biotin deficiency causing hair loss is actually rare; most “hair, skin and nails” supplements contain megadoses of biotin that interfere with lab tests without doing much for hair.
Is finasteride safe for long-term use?
For the vast majority of users, yes. Finasteride has 25+ years of post-marketing data and produces no significant long-term organ toxicity. Side effects — chiefly sexual (2-4%) and mood-related (under 1%) — usually appear in the first 6 months if at all. Patients should be counselled on the possibility of persistent post-treatment symptoms (a small but real signal) and stop the drug at the first suggestion of mood change.
Can I regrow hair without medication?
For temporary shedding (telogen effluvium, nutritional) — yes, once the cause is corrected. For androgenetic alopecia — no reliable method exists. Laser helmets, PRP, and supplements all fail to match medical therapy. Lifestyle and nutrition are essential foundations but cannot reverse the DHT pathway on their own.
How long before hair loss medication stops working?
Finasteride and minoxidil both maintain their efficacy indefinitely — but gains plateau after about 2 years. Some users notice a slow decline over 5-10 years as loss eventually overwhelms the drug effect. That’s when switching to dutasteride, or adding a second agent, is worth discussing with a dermatologist.
Is a hair transplant worth it?
For men and women at Norwood 5-7 (or Ludwig 2-3) who have stable donor hair and realistic expectations, modern transplants can produce transformative results — a natural-looking hairline and restored crown density. Cost ranges from $4,000-15,000 depending on graft count and country. Ongoing medical therapy is mandatory post-op to protect the remaining native hair.
The Bottom Line
Hair loss is one of the most-treatable cosmetic conditions in medicine — provided you get the diagnosis right, act early, and commit to the 12-month timeline. For most men with androgenetic alopecia, a combination of oral finasteride and topical minoxidil produces stabilisation in over 90% of cases. For women, minoxidil (topical or low-dose oral) plus or minus spironolactone is the equivalent foundation. Temporary shedding resolves on its own. Scarring alopecia is a dermatology emergency. Everything in between sits somewhere on a spectrum where the right treatment, started at the right time, produces the best outcome.
Browse our full hair loss product range at MedsBase — including finasteride, dutasteride, minoxidil 2% / 5% foam and solution, and oral minoxidil options. For more detailed reading, see our Finasteride vs Dutasteride comparison, Minoxidil 5% vs 10% strength guide, how to stop hair loss, and does finasteride work?
Last updated: 2026-04-17 · Reviewed by MedsBase Clinical Content Team.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.