







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
A 2024 review in the Journal of Sex Research reported that adults with little to no partnered sexual activity scored measurably lower on standard wellbeing measures than those with weekly activity, even after controlling for relationship status, age, income, and physical health. That doesn’t mean sex is a magic mood-lifter, and it doesn’t mean voluntary celibacy is bad for you. It does mean the question is worth taking seriously. In this guide we look at what the research actually shows about sexual inactivity and mental health – the hormones and neurotransmitters involved, the mood, anxiety and self-esteem signals to watch for, and what to do if a long dry spell is starting to weigh on you.
Key Takeaways
- The link is real but bidirectional – low mood reduces libido, and low intimacy can deepen low mood.
- Hormones do most of the work – oxytocin, dopamine, cortisol, and testosterone all shift with sexual activity.
- Frequency matters less than you’d think – wellbeing benefits appear to plateau around once a week.
- Voluntary celibacy is different from involuntary sexlessness – context shapes the mental-health effect.
- Treatable causes are common – erectile dysfunction, low desire, and depression often respond well to medical care.
- Non-sexual intimacy (touch, conversation, shared activity) softens most of the negative effect.
Can Sexual Inactivity Affect Your Mental Health?
Jump to a section:
- What is sexual inactivity?
- How does sexual inactivity affect mental health?
- Areas of mental health affected
- Safety profile and side effects
- What does the research say?
- Sexual inactivity vs other intimacy patterns
- What to do about it
- Frequently asked questions
- The bottom line
What Is Sexual Inactivity? (Definition & Background)
Sexual inactivity is a period of weeks, months or years without partnered sexual activity, with or without solo sexual activity. Researchers usually define it operationally as no partnered sex in the past year (sometimes the past month), but the lived experience varies widely – from a deliberate, comfortable choice to a distressing absence the person didn’t want.
That distinction matters more than the duration. A 35-year-old in a happy long-distance partnership who chooses two months without sex is not in the same position as a 35-year-old whose desire has collapsed alongside their mood. Both will show up in survey data as “sexually inactive”. Only one is likely to feel the mental-health effects. Sexual inactivity and mental health outcomes are shaped less by the calendar and more by context – desire, relationship satisfaction, physical health, and whether the inactivity was chosen or imposed.
There are several common patterns:
- Voluntary celibacy – a deliberate pause, often for religious, personal-growth, recovery, or relationship reasons.
- Involuntary sexlessness – desire is present but a partner isn’t, or sexual function isn’t.
- Sexless long-term relationships – partners are present but partnered sex has effectively stopped (commonly defined as fewer than ten times per year).
- Mismatched libido – one partner wants more sex than the other; either may end up reporting inactivity.
- Health- or medication-driven – depression, antidepressants, blood-pressure medications, and chronic illness can all reduce sexual activity even in committed couples.
Each pattern has a different mental-health profile, which is why a one-size-fits-all answer to “is sexual inactivity bad for you?” doesn’t exist.
How Does Sexual Inactivity Affect Mental Health? (Mechanism & Science)
Sexual activity changes brain chemistry in real time, and the absence of those changes – repeated over weeks and months – is what most of the proposed mental-health effects come down to.
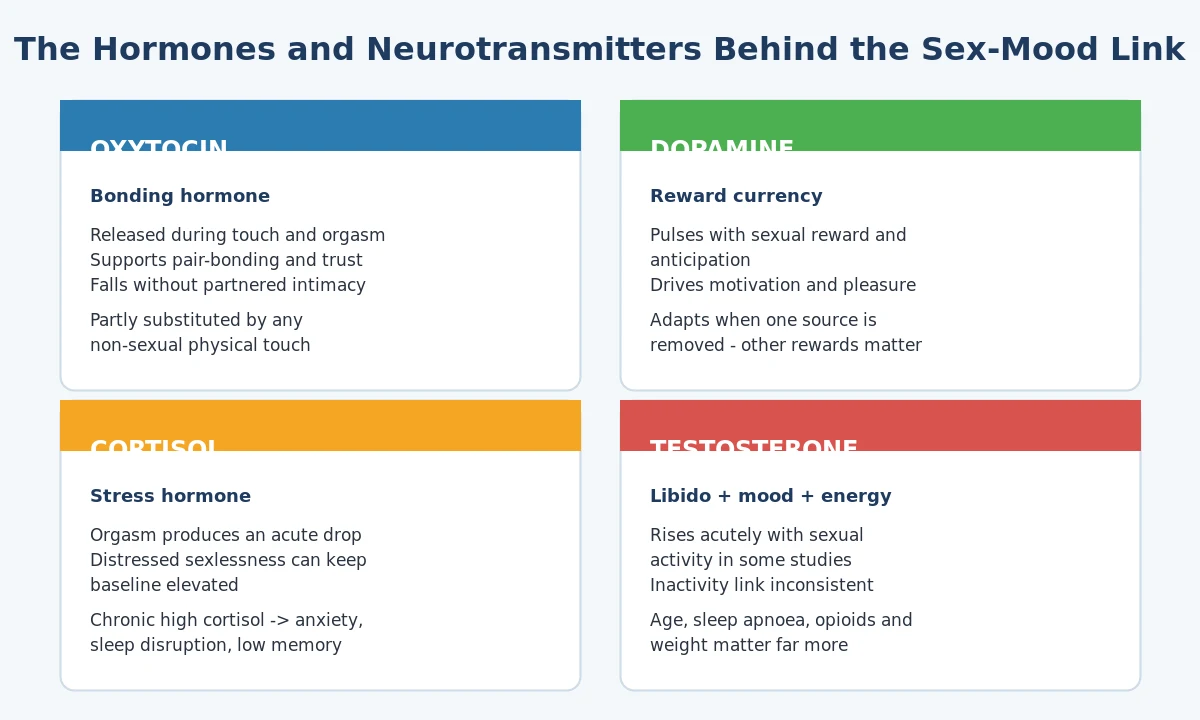
The chemistry sits across four messengers:
Oxytocin is sometimes called the bonding hormone. It rises during physical touch, orgasm, and breastfeeding, and supports pair-bonding, social trust, and a calmer stress response. Without partnered intimacy, baseline oxytocin signalling appears to drop – though touch from any source (a hug, a hand on the shoulder, a pet) can substitute partly.
Dopamine is the brain’s reward currency. Anticipating and engaging in sexual activity is one of several reliable dopamine triggers, alongside food, exercise, social connection, and creative work. The current evidence suggests dopamine signalling adapts when one source is removed, so long-term inactivity isn’t a dopamine catastrophe – but if other reward sources have also thinned out (common in depression), the cumulative effect on motivation can be real.
Cortisol is the body’s main stress hormone. Orgasm produces an acute drop in cortisol, and people in distressed sexless contexts (for example, a tense sexless marriage or chronic worry about sexual function) can show elevated baseline cortisol. Chronic high cortisol is linked with anxiety, sleep disruption, and impaired memory.
Testosterone is more complicated. Testosterone supports libido, mood, energy and bone density in both men and women, though women have far less of it. Sexual activity itself appears to nudge testosterone up acutely. Long sexual inactivity has been associated with modest declines in some studies and no change in others – the direction of cause and effect is debated.
Research Spotlight
A 2018 review in Frontiers in Psychology proposed that the mental-health benefits of sexual activity come less from the act itself than from the bundle that usually surrounds it – physical touch, emotional safety, focused attention, and a sense of being desired. Solo sexual activity captures some of these (the dopamine and stress-relief effects) but not the bonding bundle. This helps explain why people in close, affectionate sexless relationships often score better on wellbeing than people in distant, low-touch sexual ones.
The takeaway from the mechanism work: it’s rarely the absence of sex itself that drives mental-health effects. It’s the absence of the things sex tends to come with – touch, closeness, desire-being-met, and the periodic reset of the stress system.
Key Areas of Mental Health Affected by Sexual Inactivity
Several distinct mental-health domains can shift during prolonged sexual inactivity. The strength of the effect depends heavily on context – voluntary vs involuntary, satisfied vs frustrated, partnered-but-celibate vs single-and-isolated.
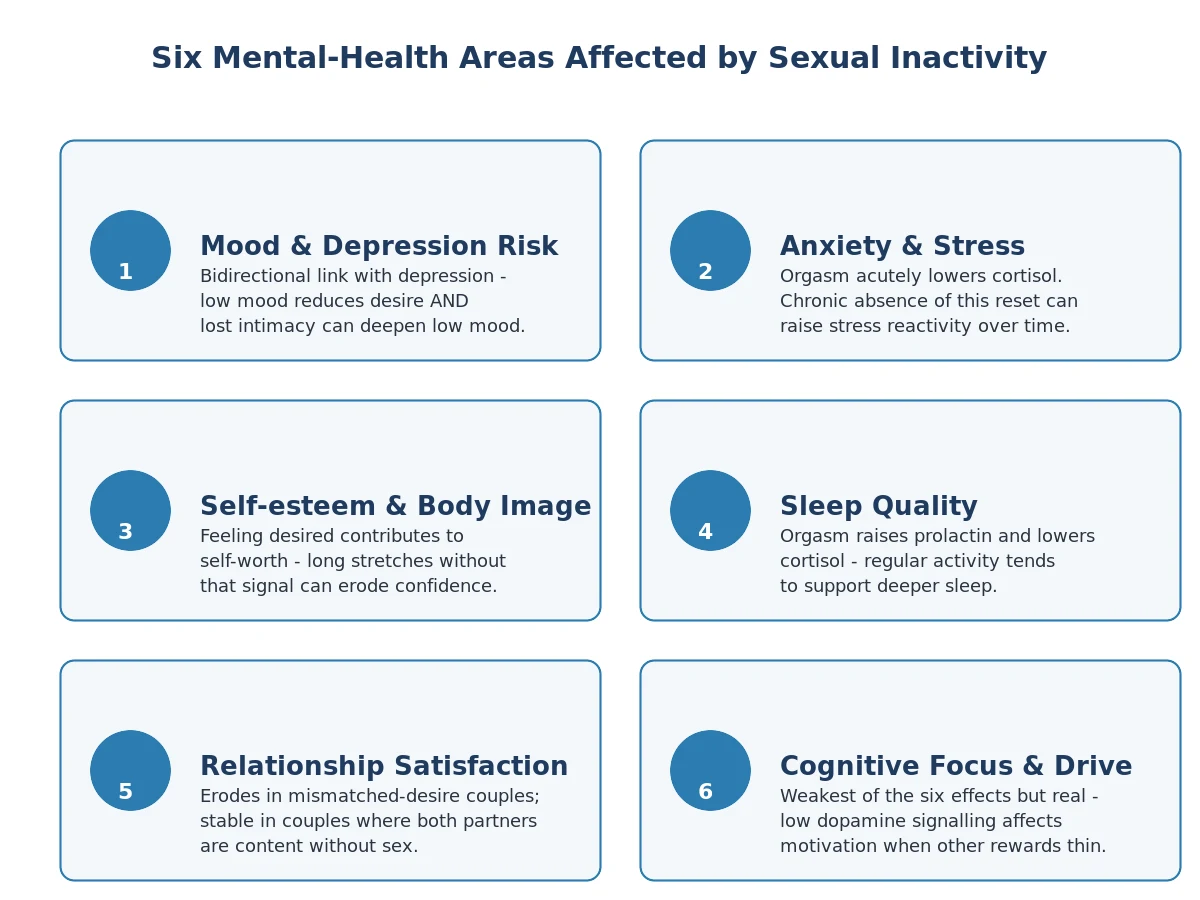
Mood and depression risk
The most consistent finding across observational studies is a modest association between higher sexual frequency and lower depression scores. Research suggests this is bidirectional: depression lowers libido (through both the illness itself and many antidepressants), and reduced intimacy can deepen low mood by removing one of the brain’s natural mood regulators. A 2017 cohort study published in Archives of Sexual Behavior reported that adults with no partnered sexual activity in the previous year had higher rates of depressive symptoms – but the authors emphasised the chicken-and-egg nature of the link.
Who Is This For?
If you’ve noticed your mood sliding alongside a long dry spell – particularly with low energy, loss of pleasure, or sleep changes lasting more than two weeks – talk to a clinician. The depression may be the cause of the inactivity rather than the consequence, and treating it tends to restore desire as well.
Anxiety and stress reactivity
Orgasm acutely reduces cortisol and increases parasympathetic (“rest and digest”) tone. Chronic absence of these resets – particularly in someone whose stress baseline is already elevated – may contribute to a more reactive anxiety profile. People in unhappy sexless relationships report higher anxiety than those in happy sexless ones; the mediator is relationship distress rather than the sexual frequency itself.
Self-esteem and body image
Feeling sexually desired contributes to many people’s sense of attractiveness and worth. A long stretch without that signal – especially after rejection, breakup or sexual difficulty – can feed into negative self-talk. This is one of the more painful but also more treatable areas: cognitive-behavioural strategies, therapy, and rebuilding non-sexual sources of self-worth all help.
Sleep quality
Orgasm raises prolactin, which has mild sedating effects, and lowers cortisol. People who report regular partnered sex tend to fall asleep faster and report deeper sleep. Solo sexual activity captures some of this, though slightly less reliably. Long inactivity isn’t a primary cause of insomnia, but it can nudge an already-fragile sleep pattern further off track.
Relationship satisfaction
In couples where both partners want sex, prolonged inactivity erodes satisfaction over time – not because of the missing sex per se, but because of the missing closeness that used to come with it, and the frustration that builds when desire goes unmet. In couples where both partners are content without sex, satisfaction can stay high indefinitely.
Cognitive focus and motivation
This is the weakest of the six domains in the evidence base, but worth mentioning. Chronic low dopamine signalling – whatever the cause – affects motivation and follow-through. If sexual activity was a meaningful piece of your reward landscape, removing it may show up as a flatter motivational state, particularly if other reward sources haven’t filled the gap.
Sexual Inactivity Safety Profile, Side Effects & “Dosage”
Calling sexual inactivity a “side-effect profile” is slightly tongue-in-cheek, but the framing is useful: what are the predictable downstream effects, how often do they occur, and how serious are they? The picture below summarises the patterns most often reported in the clinical and survey literature. Effects vary widely between individuals and the context (voluntary vs involuntary) is decisive.
| Effect | Frequency | Severity |
|---|---|---|
| Low mood / mild depressive symptoms | Common in distressed inactivity | Mild-moderate; often improves with the cause |
| Increased anxiety or stress reactivity | Common | Mild |
| Reduced self-esteem / body-image concerns | Common | Mild-moderate |
| Sleep disruption | Occasional | Mild |
| Relationship dissatisfaction (mismatched-desire couples) | Common | Moderate; can be relationship-threatening |
| Reduced libido (use-it-or-lose-it pattern) | Variable | Mild; usually reversible |
| Modest testosterone shift (some studies) | Inconsistent | Mild; clinically rarely significant |
| Pelvic-floor changes after long abstinence (post-menopause) | Occasional | Mild-moderate; treatable |
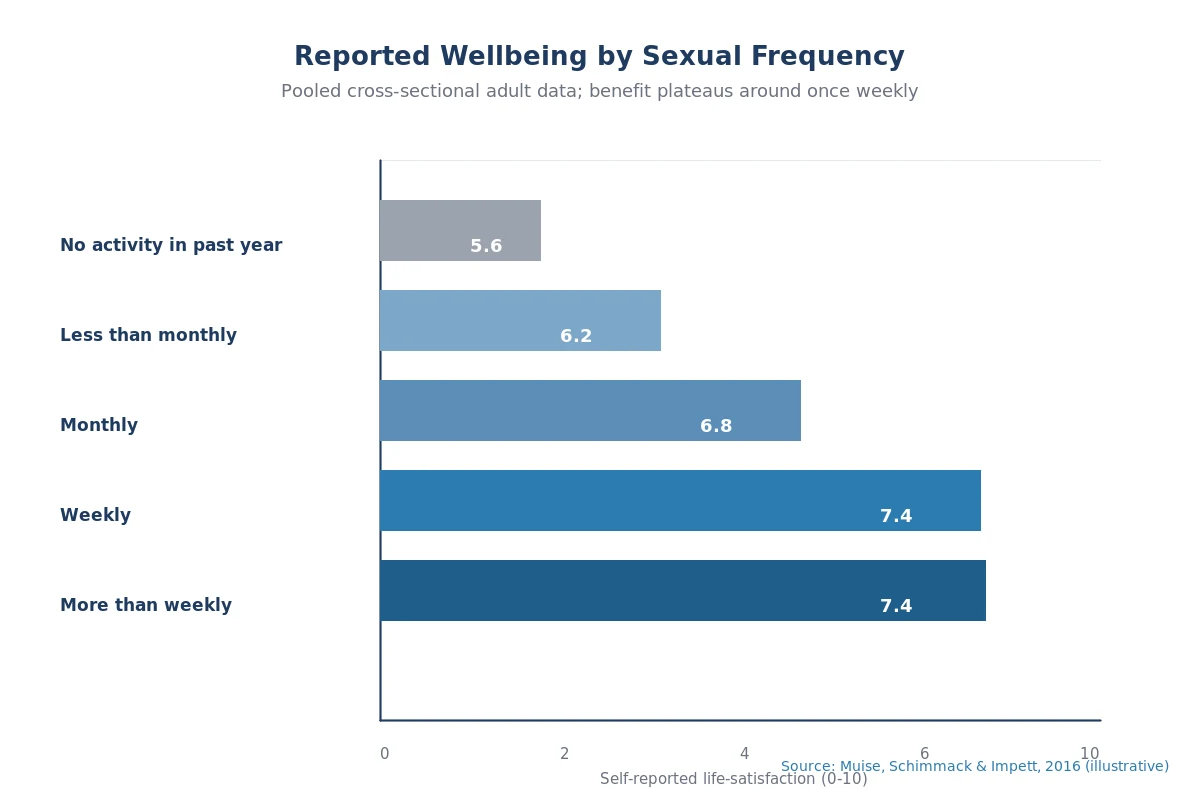
There is no clinical “dose” of sex. The closest the research comes is the Muise et al. finding that wellbeing benefits plateau around once weekly – past that, more frequent sex doesn’t measurably improve happiness or relationship satisfaction. Below that, effects vary so widely between individuals that a per-week prescription would be misleading.
What Does the Research Say?
The peer-reviewed evidence on sexual inactivity and mental health is large but uneven. Cross-sectional surveys are common, longitudinal studies are rarer, and randomised trials of sexual activity are essentially impossible to run. Below is a summary of widely-cited findings.
| Study | Year | Key finding | Source |
|---|---|---|---|
| Muise, Schimmack & Impett | 2016 | Wellbeing rises with sexual frequency up to once weekly, then plateaus. | Soc Psychol Personal Sci |
| Brody & Costa | 2008 | Higher partnered sexual frequency associated with lower depressive symptoms. | J Sex Med |
| Cao et al. | 2020 | Reduced sexual activity during pandemic lockdowns correlated with increased anxiety scores. | Psychiatry Res |
| Liu et al. (Health and Retirement Study) | 2016 | Older adults with active partnered sex showed better cognitive and emotional outcomes. | J Health Soc Behav |
| Stanton et al. | 2019 | Bidirectional link: low sexual desire predicts later depression and vice versa. | Arch Sex Behav |
| Hamilton & Meston | 2013 | Acute cortisol-lowering and parasympathetic effect of orgasm in laboratory settings. | J Sex Med |
A few qualifications are important. Most studies are observational, so they show association, not causation. People who have more sex tend to be healthier, more partnered, and less depressed for many reasons – sexual activity is one variable among many. Survey-based estimates of frequency are also self-reported and prone to over- and under-reporting. Early studies indicate the link is real and consistent, but the size of the effect is modest, and the direction of cause and effect is genuinely uncertain in many cases.
Sexual Inactivity vs Other Intimacy Patterns – Comparison
Not all “low-sex” lifestyles are mental-health-equivalent. The pattern matters more than the count.
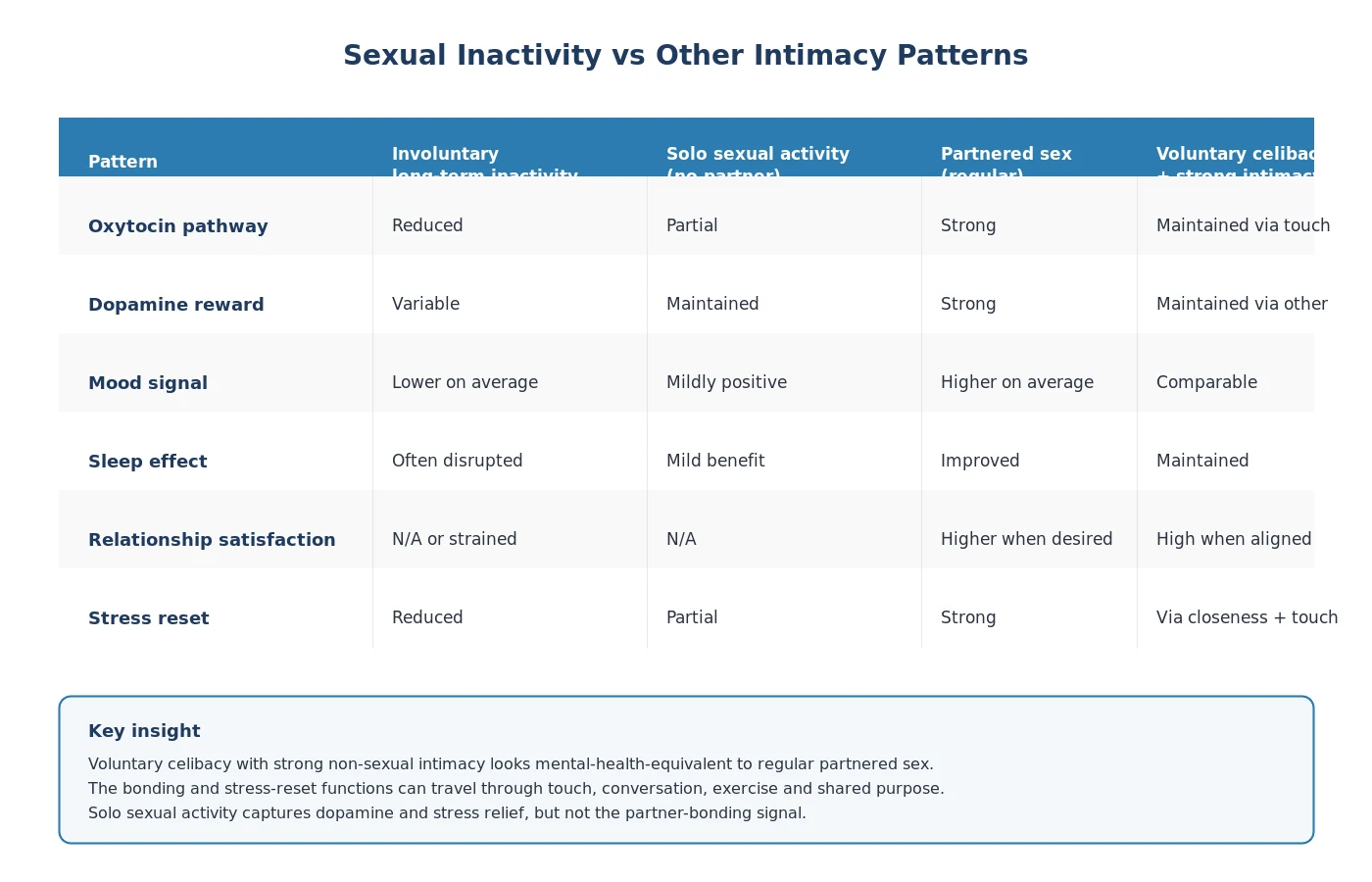
| Pattern | Oxytocin pathway | Dopamine reward | Mood signal | Relationship satisfaction |
|---|---|---|---|---|
| Involuntary long-term inactivity | Reduced | Variable | Lower on average | N/A or strained |
| Solo sexual activity, no partner | Partial | Maintained | Mildly positive | N/A |
| Partnered sex (regular) | Strong | Strong | Higher on average | Higher when desired |
| Voluntary celibacy with strong non-sexual intimacy | Maintained via touch & closeness | Maintained via other rewards | Comparable to partnered sex | High when both partners aligned |
Two patterns deserve particular note. Voluntary celibacy with strong non-sexual intimacy – for example, in long-term partnerships where both people are content without sex, or in some monastic and recovery contexts – produces wellbeing scores that are essentially indistinguishable from those of regular partnered sex. The bonding and stress-reset functions are taking other routes (touch, conversation, shared purpose, exercise, faith practice). Solo sexual activity captures some of the dopamine and stress-relief effects but not the bonding component, which is why it partly but doesn’t fully substitute for partnered sex.
How to Use This Information – Practical Guidance
If you’ve recognised yourself in any of the patterns above and want to do something about it, the path tends to follow four steps.
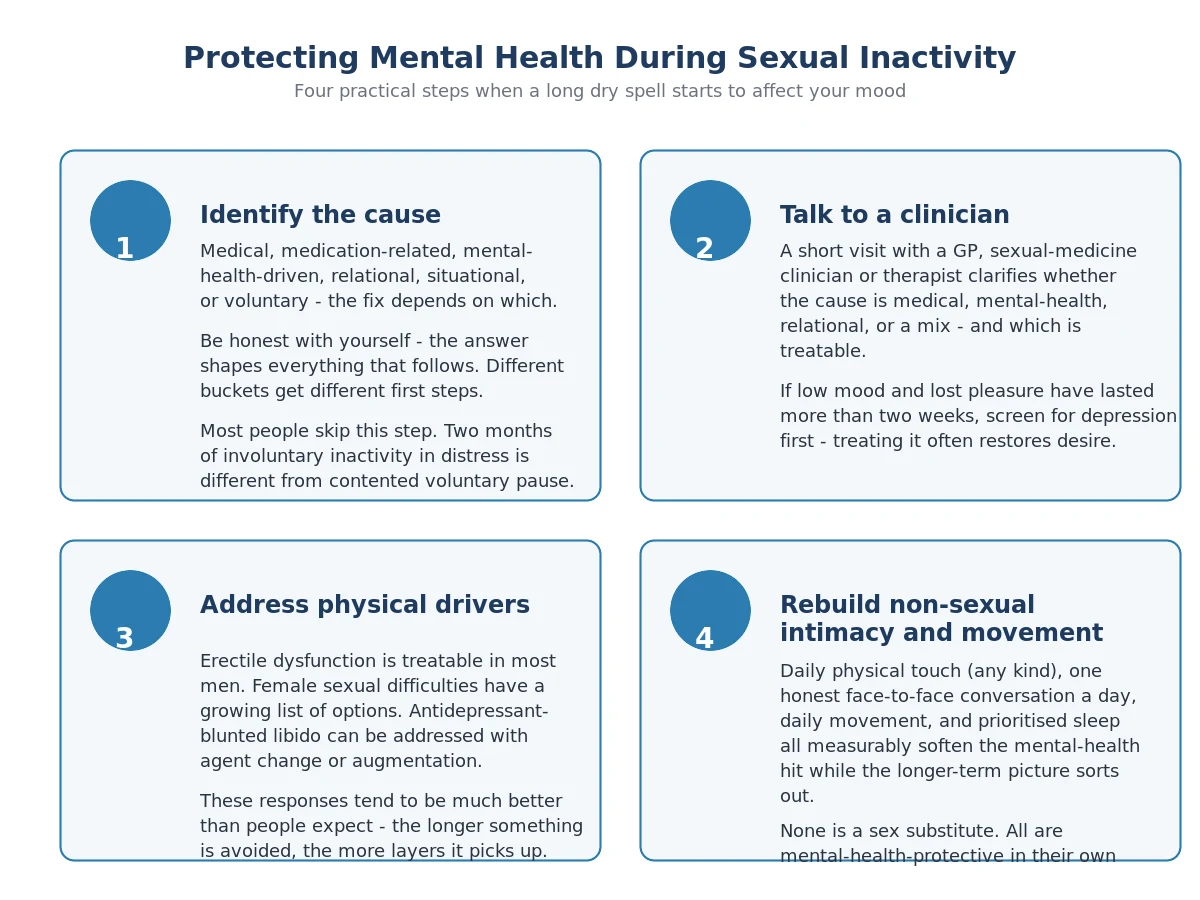
1. Identify what’s actually driving the inactivity
The fix is different depending on the cause. Write out, honestly, where you think yours sits:
- Medical (erectile or arousal difficulties, low desire, hormonal, post-illness)
- Medication-related (SSRIs, beta-blockers, finasteride, opioid pain medication)
- Mental-health-driven (depression, anxiety, trauma history)
- Relational (mismatched libido, conflict, distance, betrayal recovery)
- Situational (single, long-distance, caregiving demands, life-stage transition)
- Voluntary and welcome
The mental-health risk depends much more on which bucket applies than on how long the dry spell has been.
2. Talk to a clinician or therapist
This is the step people most often skip. A short conversation with a GP, sexual-medicine clinician or psychotherapist can clarify whether the cause is medical, psychological, relational, or a mix – and which of those is treatable. If mood symptoms are present (low energy, lost pleasure, sleep change, hopelessness lasting more than two weeks), screen for depression first; treating the depression often restores desire.
3. Address treatable physical factors
Many of the most common drivers of involuntary sexlessness respond well to treatment. Erectile dysfunction is treatable in the majority of men with PDE5 inhibitors such as sildenafil, tadalafil and vardenafil (browse our erectile dysfunction medication range). Female sexual dysfunction has fewer evidence-based pharmacological options but several work for specific subtypes – explore the female sexual dysfunction category for what’s currently available. Where antidepressants are blunting libido, switching agents or adding bupropion is an evidence-based option that should be discussed with a prescriber rather than self-managed; relevant products live in the mental health and psychiatric medications section. For premature ejaculation specifically, dapoxetine and other SSRIs sit in the premature ejaculation treatment category.
4. Rebuild non-sexual intimacy and movement
Even before any sexual issue is resolved, the bonding and stress-reset functions can be partially recovered through other channels. The evidence for each of these is consistent if not dramatic: regular physical touch (even non-sexual – hugs, hand-holding, a hand on the back), at least one face-to-face honest conversation per day with someone who matters to you, daily movement of any kind, and sleep prioritisation. None of these is a sex substitute. All of them are mental-health protective in their own right and tend to make the eventual return to sexual activity easier.
Research Spotlight
A 2021 trial in Psychosomatic Medicine reported that adults randomised to a four-week daily-touch protocol with their partners (no sexual content required) showed measurable reductions in cortisol and self-reported anxiety compared with controls. The implication: many of the stress-physiology benefits associated with sex can be partially captured by intentional, non-sexual physical closeness.
Frequently Asked Questions
Can not having sex cause depression?
Research suggests the link between sexual inactivity and depression is real but bidirectional and modest in size. Lack of partnered sex doesn’t directly cause clinical depression in someone whose mood was previously stable, but it can deepen low mood in someone already vulnerable, particularly when the inactivity is involuntary and accompanied by relationship distress. Conversely, depression itself reduces desire – so the inactivity is often the symptom, not the cause. If low mood lasts more than two weeks alongside loss of pleasure, sleep change, or fatigue, talk to a clinician.
How long is too long without sex?
There is no clinical threshold. Wellbeing benefits of partnered sex appear to plateau around once weekly in survey data, but plenty of adults report excellent mental health with far less. The more relevant question is whether the inactivity feels chosen and comfortable or unwanted and distressing. Two months of involuntary inactivity in a frustrated person may have more mental-health impact than a year of contented voluntary celibacy.
Does sexual inactivity lower testosterone?
Some studies show modest declines in testosterone after long stretches of sexual inactivity in men, while others show no change or even short-term increases after brief abstinence. The effect, if real, is small and inconsistent. Clinically meaningful low testosterone is much more likely to be driven by ageing, obesity, sleep apnoea, opioid use, or pituitary issues than by a dry spell. If you suspect low testosterone, ask a clinician for a morning total-testosterone blood test rather than self-diagnosing from libido alone.
Is voluntary celibacy bad for your mental health?
Available evidence suggests no. Adults in voluntary celibacy with strong non-sexual social and physical connection – long-term partnerships, monastic life, recovery contexts – report wellbeing scores comparable to those of sexually active adults. The mental-health risk is concentrated in involuntary inactivity accompanied by frustration, relationship distress, or low mood, not in chosen abstinence.
Can a sexless relationship cause depression in either partner?
It can, particularly when one partner wants sex and the other doesn’t. The mechanism is rarely the missing sex itself – it’s the missing closeness, the build-up of unmet desire, and the erosion of feeling wanted. Couples where both partners are content without sex tend to maintain high satisfaction and low depression rates. Couples therapy that addresses underlying conflict, desire mismatch, or untreated sexual dysfunction is often more effective than focusing on frequency.
Does masturbation help if I’m not having partnered sex?
Solo sexual activity captures some of the mental-health benefits associated with partnered sex – the dopamine pulse, the cortisol drop, sleep effects – but not the bonding component mediated by oxytocin and partner contact. Research suggests it partially substitutes for partnered sex on mood and stress, particularly for people who don’t currently have a partner. It’s not a one-for-one replacement and won’t address the loneliness piece for someone who wants connection.
I’m avoiding sex because of erectile difficulties. What should I do?
This is one of the most common and most treatable drivers of involuntary sexlessness in men over 40. Erectile dysfunction is usually treatable, and the longer it’s avoided the more performance anxiety tends to layer on top. A clinician visit is the right first step – they’ll screen for cardiovascular causes (ED is often the earliest sign of vascular disease), review medications, and discuss treatment. PDE5 inhibitors such as sildenafil and tadalafil are first-line for most men. Browse our erectile dysfunction medication range if you’d like to see what’s available alongside that conversation.
When should I see a doctor about sexual inactivity?
If any of the following apply: low mood, loss of pleasure, or sleep change for more than two weeks; erectile, arousal or orgasm difficulties that have lasted more than three months; sudden change in libido without an obvious cause; pain with sex; or distress in your relationship that you can’t find a way through. A clinician can usually distinguish in one or two visits between a medical, hormonal, mental-health, and relational driver – and the treatment path depends entirely on which it is.
The Bottom Line
The relationship between sexual inactivity and mental health is real, modest, and shaped much more by context than by the calendar. Voluntary celibacy with rich non-sexual intimacy looks mental-health-neutral in the data. Involuntary inactivity in someone whose desire is frustrated – particularly when it’s tangled up with depression, an untreated sexual difficulty, or a strained relationship – is where the meaningful risk sits.
The good news is that the most common drivers are treatable. Depression responds to therapy and to evidence-based medication. Erectile dysfunction responds to first-line medications in the majority of men. Mismatched libido in couples often responds to honest conversation and, where needed, sex-positive couples therapy. And in the meantime, the simpler protective behaviours – daily touch, daily honest conversation, daily movement, prioritised sleep – measurably soften the mental-health hit while you sort out the longer-term picture.
If something in this article matched your situation more closely than you’d like, the right next step is rarely “wait it out”. It’s a short conversation with a clinician, a therapist, or your partner – depending on which bucket you sit in.
Last updated 29 April 2026. Our editorial process draws on peer-reviewed sources including the Journal of Sex Research, Archives of Sexual Behavior, NHS, and PubMed-indexed clinical literature.
Medical disclaimer. This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis or treatment. Sexual health concerns, mood symptoms lasting more than two weeks, and relationship distress all benefit from individualised assessment by a qualified clinician. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this page.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.