







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

Reviewed by the MedsBase Editorial Team · Last updated: April 17, 2026
More than two-thirds of adults under 50 carry HSV-1, and roughly one in six adults aged 14–49 carries HSV-2, according to the World Health Organization. For most people, the practical question isn’t whether they’ll ever need a herpes antiviral — it’s which one. If your doctor has mentioned valacyclovir vs acyclovir, you’ve landed on the two drugs that dominate modern antiviral prescribing for cold sores, genital herpes, shingles, and chickenpox.
These two medications are closely related — so closely, in fact, that valacyclovir is literally converted into acyclovir inside your body. But the practical differences between them (dosing frequency, how much drug actually reaches your bloodstream, cost, and convenience) matter more than most patients realise. This guide walks through the clinical evidence, the real-world trade-offs, and how to decide which is right for your situation.
- Valacyclovir is a prodrug of acyclovir — once absorbed, your body converts it into the same active molecule.
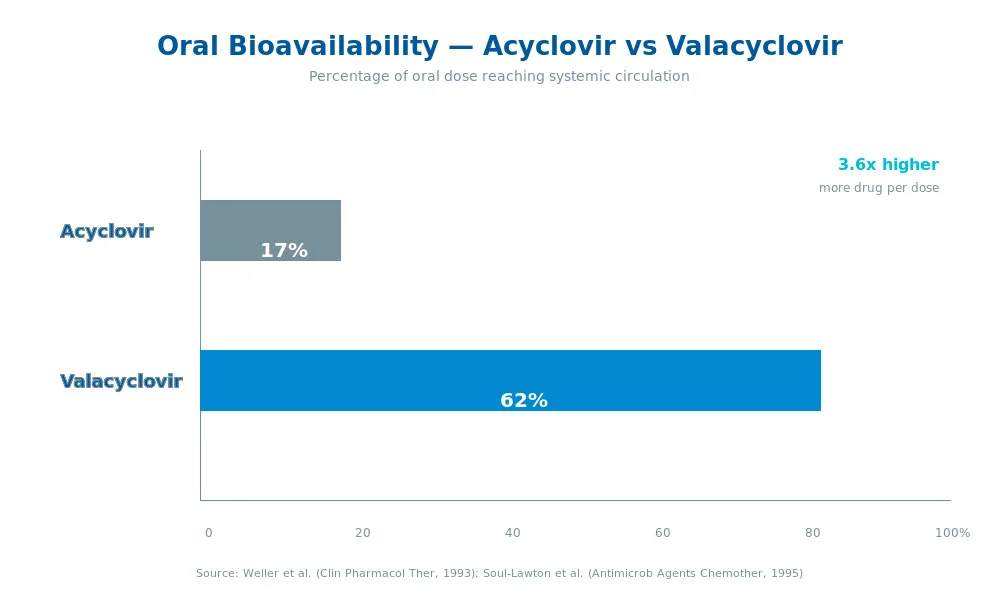
- Valacyclovir’s oral bioavailability is 3–5× higher than acyclovir’s, meaning fewer tablets per day.
- Both drugs are equally effective against HSV-1, HSV-2, and VZV when dosed appropriately.
- Acyclovir typically costs less as a generic; valacyclovir offers simpler dosing.
- Both are generally well tolerated, but both require dose adjustment in kidney disease.
- Only valacyclovir has FDA-approved data showing reduced HSV-2 transmission to partners.
Valacyclovir vs Acyclovir — Which Antiviral Actually Works Better in 2026?
What Are Valacyclovir and Acyclovir?
Quick Answer — What is Valacyclovir vs Acyclovir?
Valacyclovir and acyclovir are both antiviral medications used to treat herpes simplex (HSV-1 and HSV-2) and varicella-zoster (VZV) infections. Acyclovir is the original antiviral molecule; valacyclovir is its prodrug — an L-valyl ester that converts into acyclovir inside the body but absorbs far more efficiently from the gut.
Acyclovir was introduced in 1982 by Burroughs Wellcome. It was the first clinically useful antiviral with true selectivity for infected cells, and its discoverer Gertrude Elion shared the 1988 Nobel Prize in Physiology or Medicine for the work that led to it. Acyclovir remains a World Health Organization Essential Medicine in 2026.
Valacyclovir was approved by the FDA in 1995 under the brand name Valtrex. Chemists at Glaxo (later GSK) attached the amino acid L-valine to acyclovir, producing a compound that gut and liver enzymes quickly snip back apart — releasing free acyclovir into the bloodstream. The result: a drug that’s pharmacologically identical to acyclovir once absorbed, but far more convenient to dose.
Both drugs are now widely available as generics under brand names including Zovirax, Valtrex, Valclovir, Ekovir, and others. MedsBase stocks multiple generic options for both molecules.
A brief history of antiviral development
Before acyclovir, antiviral therapy was a frontier with almost no reliable options. Earlier compounds like vidarabine and idoxuridine had severe toxicity because they couldn’t distinguish between viral and human DNA replication. Acyclovir solved that selectivity problem in a single molecular stroke, and that breakthrough is why herpes infections — once managed largely with topical creams and patience — became reliably controllable with an oral pill.
The 13-year gap between acyclovir’s launch (1982) and valacyclovir’s launch (1995) reflects a classic second-generation drug development pattern. Once the parent molecule proved both safe and effective, pharmaceutical chemistry focused on solving its biggest practical weakness — poor oral absorption. The valyl ester “prodrug” strategy has since been applied to many other antivirals, including the HIV drug tenofovir alafenamide and the influenza drug oseltamivir.
How Do Valacyclovir and Acyclovir Work?
Both drugs are guanosine analogs — molecular look-alikes of one of the four DNA building blocks. They exploit a neat trick: they’re only activated inside cells that are already infected with a herpes-family virus.
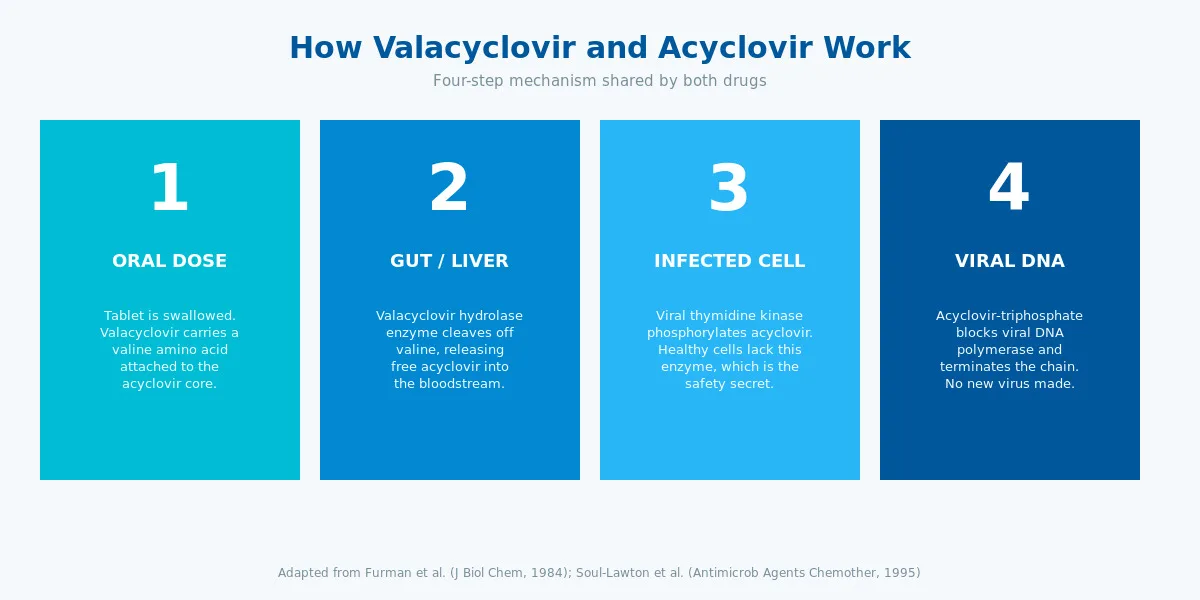
Here’s the three-step mechanism:
- Selective activation. Herpes-infected cells contain a viral enzyme called thymidine kinase (TK). This enzyme grabs acyclovir and attaches a phosphate group. Human cells don’t have viral TK, so the drug stays inactive in healthy tissue — which is the secret to acyclovir’s excellent safety profile.
- Second and third phosphorylation. Host cell enzymes add two more phosphates, producing acyclovir triphosphate — the active form.
- DNA chain termination. Acyclovir triphosphate fools the viral DNA polymerase into using it instead of real guanosine. Once incorporated, it cannot be extended — the growing viral DNA chain is permanently terminated. Viral replication halts.
The single most important pharmacokinetic difference between the two drugs lives at step zero, before any of this happens: getting the drug out of the gut and into the blood. This is where valacyclovir’s engineered advantage kicks in, and it’s the reason most modern prescribers default to valacyclovir when cost isn’t a barrier.
Why the prodrug strategy matters
Plain acyclovir has a structural quirk that hurts its absorption. It lacks a natural amino-acid transporter on the gut wall, so most of a swallowed dose passes through unabsorbed. Valacyclovir bypasses that limit by hitching a ride on the body’s peptide transporter, PEPT1, which is designed to move dipeptides across the gut lining at high speed.
Once absorbed, the valyl ester bond is snipped by a hepatic enzyme called valacyclovir hydrolase. Within minutes, free acyclovir flows into the systemic circulation. From that point onward, the pharmacology is identical — which is why switching between the two drugs is a matter of dose arithmetic, not a change in mechanism.
This is also why resistance patterns are identical between the two drugs. Any strain of HSV or VZV that becomes resistant to acyclovir is automatically resistant to valacyclovir, because both deliver the same active molecule. Resistance is rare in immunocompetent patients but emerges in roughly 5% of severely immunocompromised patients — mostly those with advanced HIV or post-transplant status.
Key Uses & Applications
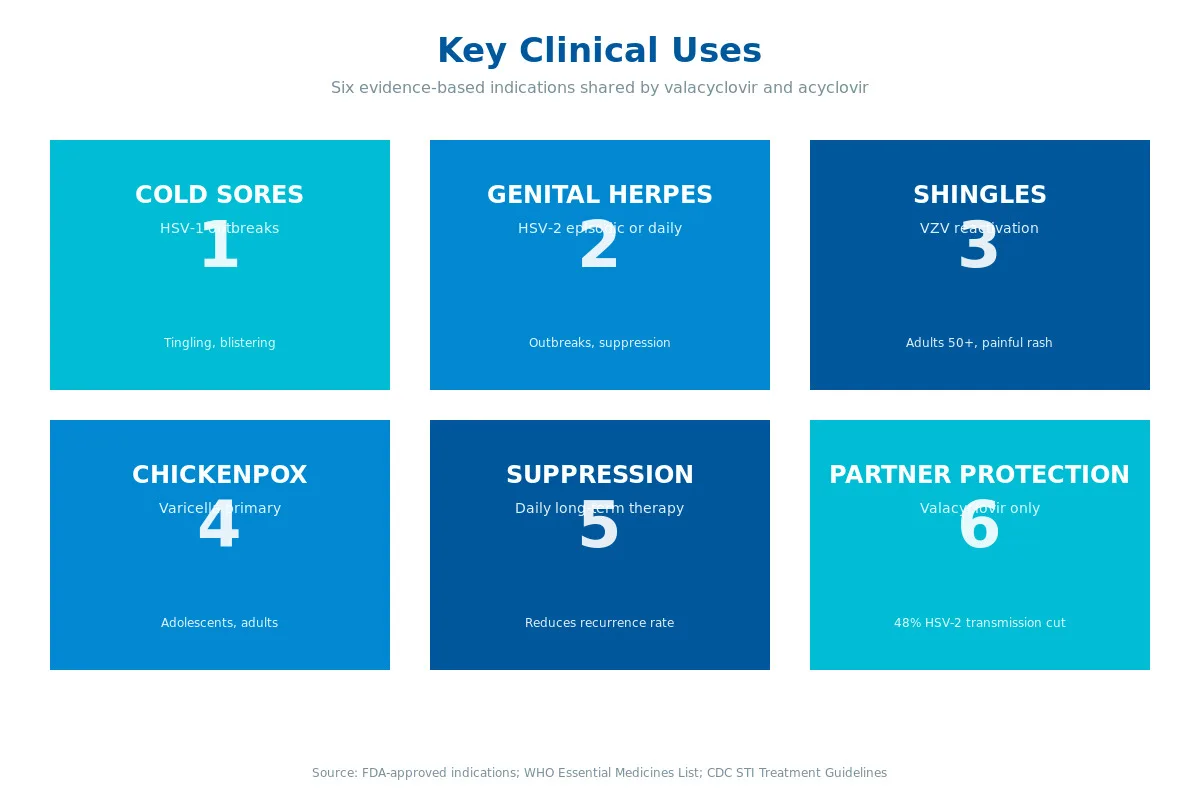
Infographic summary: Cold Sores (HSV-1 outbreaks) · Genital Herpes (HSV-2 episodic or daily) · Shingles (VZV reactivation in adults 50+) · Chickenpox (varicella primary infection) · Daily Suppression (reduces HSV recurrence rate) · Partner Protection (valacyclovir-only — 48% HSV-2 transmission reduction).
Both drugs share the same FDA-approved indications. Clinicians generally choose between them based on convenience, cost, and patient preference — not clinical effectiveness.
HSV-1 (Cold Sores / Oral Herpes)
Cold sores — the tingly, blistering outbreak on or near the lip — are caused mostly by HSV-1. Both drugs shorten outbreak duration when started at the first prodromal tingle.
- Valacyclovir: 2 g twice daily for one day (single-day therapy).
- Acyclovir: 400 mg five times daily for 5 days.
The single-day valacyclovir protocol — pioneered in Spruance et al. (2003) — is a clear win for quality of life, especially if you travel or struggle with complex dosing schedules.
HSV-2 (Genital Herpes)
Here both drugs play two different roles: episodic therapy (treat an outbreak when it flares) and suppressive therapy (take daily to prevent recurrences).
- Episodic — Valacyclovir: 500 mg twice daily × 3 days.
- Episodic — Acyclovir: 400 mg three times daily × 5 days.
- Suppressive — Valacyclovir: 500 mg–1 g once daily.
- Suppressive — Acyclovir: 400 mg twice daily.
Herpes Zoster (Shingles)
Shingles requires higher doses and earlier starts to reduce the risk of post-herpetic neuralgia — the long-lasting nerve pain that can follow a shingles outbreak.
- Valacyclovir: 1 g three times daily × 7 days.
- Acyclovir: 800 mg five times daily × 7–10 days.
In a head-to-head trial, Beutner et al. (1995) found valacyclovir significantly shortened zoster-associated pain vs acyclovir in immunocompetent adults over 50. For shingles specifically, the evidence base tilts toward valacyclovir — but the Shingrix vaccine, when available, is a superior first-line prevention strategy for adults 50+ and should always be discussed first.
Varicella (Chickenpox)
Both drugs are used — usually in adolescents and adults, where chickenpox tends to be more severe than in young children. Early antiviral therapy (within 24 hours of rash onset) shortens illness by 1–2 days and reduces complication risk. In children under 12, the decision to treat is individualized; routine treatment of uncomplicated paediatric chickenpox is not standard because most cases resolve without intervention.
Immunocompromised Patients and Transplant Recipients
Long-term antiviral prophylaxis in stem-cell and solid-organ transplant is an important niche, where valacyclovir’s once- or twice-daily dosing simplifies already complex medication regimens.
Safety Profile, Side Effects & Dosage
Both drugs have been prescribed to hundreds of millions of people across four decades. Their safety profile is one of the best-characterised in modern pharmacology.
Common and Rare Side Effects
| Side effect | Frequency | Severity |
|---|---|---|
| Headache | Common (≥10%) | Mild |
| Nausea | Common (5–10%) | Mild |
| Abdominal pain | Common (3–5%) | Mild |
| Dizziness | Uncommon (1–3%) | Mild |
| Fatigue | Uncommon (1–3%) | Mild |
| Rash | Uncommon (<1%) | Mild–moderate |
| Acute kidney injury (crystal nephropathy) | Rare | Serious — reversible |
| Neurotoxicity (confusion, tremor, hallucinations) | Rare | Serious — elderly / CKD risk |
| Thrombotic thrombocytopenic purpura (TTP) | Very rare | Serious — in severe immunocompromise |
Dose Adjustment in Kidney Disease
Both drugs are renally excreted, and both require dose reduction when creatinine clearance drops below ~50 mL/min. This is the single most common source of adverse events — routinely check renal function before prescribing to older adults.
Drug Interactions
Clinically meaningful interactions are few. Caution is warranted with other nephrotoxic drugs (NSAIDs at high dose, aminoglycosides, IV contrast) and with cimetidine or probenecid, which slow acyclovir clearance.
Pregnancy and Breastfeeding
Both drugs are categorized as generally compatible with pregnancy, and there is a large registry dataset supporting this. Acyclovir has the longer track record simply because it has existed longer — but valacyclovir data is now also extensive and reassuring. Always consult a prescriber; never self-prescribe in pregnancy.
What Does the Research Say?
The evidence base is unusually mature for these two drugs — here are five landmark studies worth knowing.
| Study | Year | Finding | Source |
|---|---|---|---|
| Weller et al. | 1993 | Acyclovir oral bioavailability ≈ 15–20% | Clin Pharmacol Ther |
| Soul-Lawton et al. | 1995 | Valacyclovir produces plasma acyclovir AUCs equivalent to IV acyclovir | Antimicrob Agents Chemother |
| Beutner et al. | 1995 | Valacyclovir accelerated shingles pain resolution vs acyclovir in adults 50+ | Antimicrob Agents Chemother |
| Spruance et al. | 2003 | Single-day valacyclovir 2 g BID shortens cold sore outbreaks vs placebo | Antimicrob Agents Chemother |
| Corey et al. | 2004 | Daily valacyclovir reduced HSV-2 transmission to susceptible partners by ≈ 48% | NEJM |
Research suggests the clinical effectiveness of the two drugs is essentially equivalent once acyclovir is actually delivered to infected cells — the practical differences come from absorption and dosing convenience.
Early studies indicate that valacyclovir’s once- or twice-daily dosing substantially improves patient adherence in chronic suppressive therapy vs acyclovir’s multi-daily regimens. Better adherence means fewer breakthrough outbreaks in real-world use.
The Corey et al. (2004) transmission study is particularly notable because it gave valacyclovir a partner-protection indication that acyclovir doesn’t carry — making valacyclovir the default choice for serodiscordant couples.
What about long-term suppression?
For people with six or more recurrent outbreaks per year, daily suppressive therapy is the evidence-based recommendation. Long-term studies have followed patients on continuous acyclovir for 10+ years and continuous valacyclovir for 6+ years without meaningful safety signals or loss of effectiveness. Goldberg et al. (1993) observed patients on daily acyclovir for up to a decade and reported a steady reduction in outbreak frequency without drug accumulation or organ toxicity. That dataset remains the gold-standard reassurance for long-term suppressive therapy.
Recurrence-free rates in the original suppressive-therapy trials were roughly 70–85% over a year of treatment, with partial protection even after discontinuation — patients often experience fewer outbreaks in the months following a long suppressive course, likely because continuous viral suppression allows the immune system to regain the upper hand.
Valacyclovir vs Acyclovir — Head-to-Head Comparison
Here’s the practical side-by-side.
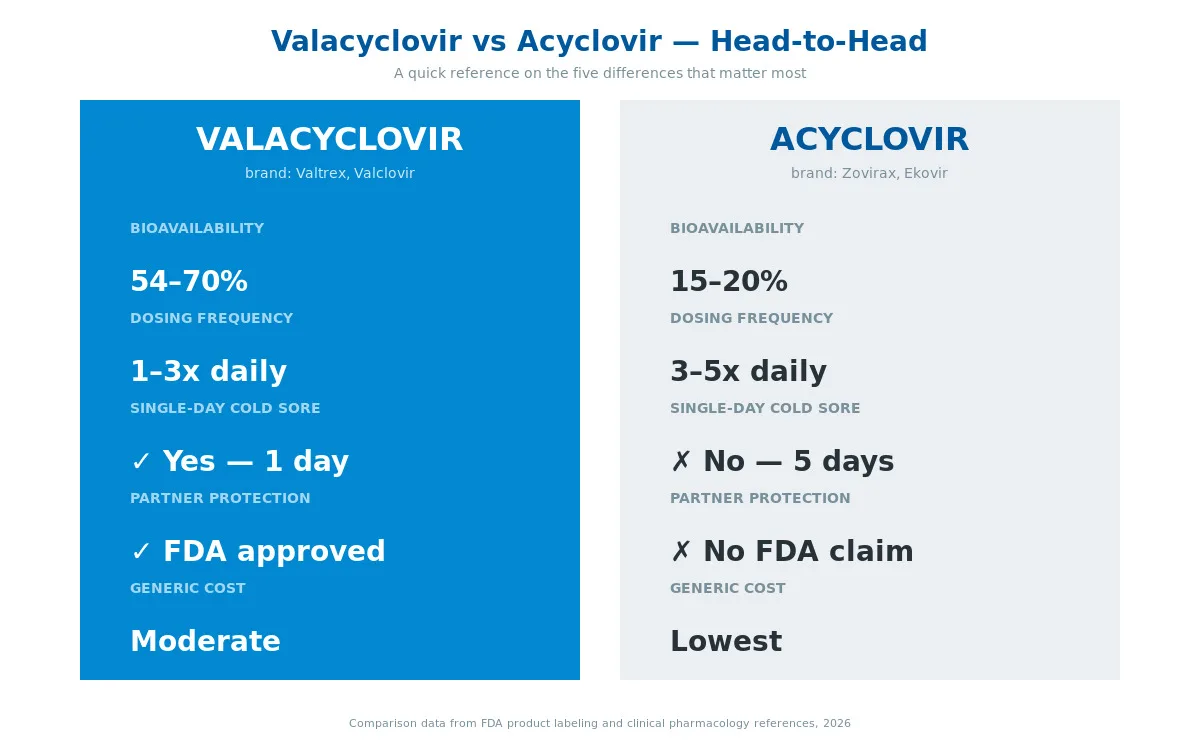
| Criterion | Valacyclovir | Acyclovir |
|---|---|---|
| FDA approval year | 1995 | 1982 |
| Drug class | Nucleoside analog prodrug | Nucleoside analog |
| Oral bioavailability | 54–70% | 15–20% |
| Dosing frequency (typical) | 1–3× daily | 3–5× daily |
| Single-day cold sore therapy? | Yes (2 g BID × 1 day) | No (5-day course) |
| FDA indication for HSV-2 transmission reduction? | Yes | No |
| IV formulation available? | No | Yes (for severe/systemic) |
| Generic cost (typical) | Moderate | Low |
| Renal dose adjustment needed? | Yes | Yes |
| Pregnancy safety data | Extensive | Most extensive |
| Mechanism of action | Converts to acyclovir; then identical | Direct |
Bottom line on the head-to-head: valacyclovir is more convenient and carries the transmission-reduction claim; acyclovir is cheaper and has the longest safety track record plus an IV option for hospital use. Neither is “stronger” — they’re the same active molecule once absorbed.
What about famciclovir — a third option?
A common follow-up question: if valacyclovir and acyclovir are the two main players, what is famciclovir (brand name Famvir) doing in the picture? Famciclovir is a prodrug of penciclovir — a different guanosine analog with a similar but not identical mechanism. It offers dosing and efficacy broadly comparable to valacyclovir and is a reasonable third-line choice in patients who don’t tolerate either acyclovir or valacyclovir.
Head-to-head trials have generally shown valacyclovir and famciclovir to be clinically interchangeable for genital herpes and shingles. Price, availability, and prescriber familiarity usually decide which one is chosen. Famciclovir is not stocked as widely as valacyclovir on most international pharmacy sites.
When should your prescriber consider IV acyclovir?
Oral therapy is adequate for most herpes infections. IV acyclovir, which only acyclovir (not valacyclovir) offers, is reserved for life-threatening or deep-tissue infections — herpes encephalitis, neonatal herpes, disseminated varicella in immunocompromised hosts, or severe HSV complications in transplant patients. In those settings, IV dosing achieves the high plasma concentrations needed to penetrate the central nervous system or deep organs, and the oral route simply isn’t fast or high enough.
How to Take Valacyclovir or Acyclovir Correctly
Three universal rules apply to both drugs:
- Start dosing as early as possible. Antivirals work by blocking ongoing viral replication. Starting within 24–72 hours of the first symptom (tingle, prodrome, first blister) produces the biggest clinical benefit. Starting late reduces efficacy dramatically.
- Complete the full course. Stopping early because symptoms improve allows viral rebound and may increase relapse risk. For suppressive therapy, consistency is everything.
- Hydrate well. Both drugs crystallise in the kidney if you’re dehydrated. Drink water throughout the course — especially at higher zoster and single-day cold-sore doses.
Practical tips
- Food doesn’t matter much. Valacyclovir absorption is unaffected by food; acyclovir absorption varies mildly. Either can be taken with or without meals.
- Don’t double up missed doses. If you miss one, take it as soon as you remember unless the next dose is within a couple of hours.
- Store at room temperature, away from moisture. No refrigeration needed.
- Watch for confusion or tremor in older adults — these are signs of neurotoxicity that warrants urgent dose review.
Browse our full range of valacyclovir and acyclovir generic medications — including Valclovir, Valovera, Valcosign, Centrex, and Ekovir — all shipped discreetly worldwide. For broader context, see our guide on how aciclovir works in treatment of genital herpes.
Frequently Asked Questions
Is valacyclovir stronger than acyclovir?
Valacyclovir is not “stronger” in a pharmacological sense — it converts into the same active molecule (acyclovir) once absorbed. What valacyclovir offers is higher oral bioavailability (54–70% vs 15–20%), which means more active drug reaches your bloodstream from each dose. Clinically, this translates to fewer pills per day, not a more potent effect at the infection site.
Can I take valacyclovir instead of acyclovir if my doctor prescribed acyclovir?
Only after speaking with your prescriber. The two drugs are clinically equivalent when dosed correctly, but the doses are different — swapping one for the other at the same number of milligrams will give you a very different exposure. Your doctor or pharmacist can convert the regimen safely if cost, tolerability, or convenience warrants the switch.
Which is better for cold sores — valacyclovir or acyclovir?
For most otherwise-healthy adults, valacyclovir wins on convenience — a single-day, two-dose regimen (2 g BID × 1 day) is substantially easier than acyclovir’s 5-day, five-times-daily course. Clinical outcomes are similar when both are started early. If cost is the deciding factor, acyclovir remains a perfectly effective option.
How fast does valacyclovir work compared to acyclovir?
Both drugs begin suppressing viral replication within hours of the first dose. Symptom-relief timelines look similar in head-to-head studies — typical cold-sore healing time drops by 1–2 days with either drug, compared to untreated outbreaks. The bigger determinant of response speed is how early you start treatment, not which drug you chose.
Is valacyclovir safer than acyclovir?
The side-effect profiles are essentially identical because you end up with acyclovir in your bloodstream either way. Acyclovir has a longer real-world safety track record simply because it has been prescribed since 1982. Both require dose reduction in kidney disease, and both can rarely cause neurotoxicity in older adults or those with renal impairment.
Why is valacyclovir more expensive than acyclovir?
Valacyclovir was patented later (1990s), so its generic market is younger and unit prices haven’t fully converged to acyclovir’s. Acyclovir is one of the cheapest prescription antivirals in the world. That price gap is narrowing steadily — at MedsBase, generic valacyclovir brands like Valclovir and Valovera are priced close to generic acyclovir options.
Can valacyclovir prevent spreading herpes to my partner?
Yes — this is one of valacyclovir’s distinguishing claims. A landmark 2004 NEJM study (Corey et al.) showed daily suppressive valacyclovir reduced HSV-2 transmission to uninfected partners by roughly 48%. This indication is specifically FDA-approved for valacyclovir and is a major reason it’s preferred in serodiscordant couples.
Do I need a prescription for valacyclovir or acyclovir?
Yes. In almost every country both drugs are prescription-only. A prescriber will assess your symptoms, kidney function, and any pregnancy status before recommending a dose and duration. Never self-prescribe antivirals — incorrect dosing wastes the therapeutic window and occasionally causes harm.
The Bottom Line
The valacyclovir vs acyclovir decision is rarely about which drug is “better” — they’re the same active molecule once absorbed. The real choice is between valacyclovir’s convenience (fewer pills, simpler schedules, the transmission-reduction claim for couples) and acyclovir’s cost (decades of generic pricing and the longest safety record).
For most cold-sore and genital-herpes patients who can afford either, modern prescribers default to valacyclovir. For price-sensitive patients, long-term suppression on a budget, or IV therapy in hospital, acyclovir is the right answer. Both belong in your doctor’s toolkit — and MedsBase stocks generics of both across a wide range of strengths and pack sizes.
Ready to explore your options? Browse our full antiviral catalogue or speak to your healthcare provider about which regimen fits your situation.
Decision summary — how most prescribers actually choose
If you want a one-paragraph heuristic that mirrors how experienced prescribers think about this in 2026:
- Episodic therapy (one-off outbreak): valacyclovir for convenience; either drug for cost-sensitive patients.
- Long-term daily suppression: valacyclovir once daily is the modern default for adherence. Acyclovir twice daily is a reasonable cost-driven alternative.
- Serodiscordant couples (partner HSV-2 negative): valacyclovir daily, because of its FDA-backed transmission-reduction data.
- Shingles in an adult 50+: valacyclovir first-line; Shingrix vaccination is a higher-priority conversation for future prevention.
- Severe systemic infection: IV acyclovir in hospital.
- Pregnancy: either drug is considered safe; acyclovir has the longer registry track record but valacyclovir data is now extensive.
Whatever regimen you’re prescribed, the two rules that predict success are the same: start early, and don’t miss doses. Both drugs lose efficacy dramatically when started more than 72 hours after symptoms begin, and any missed doses during suppressive therapy can give the virus an opportunity to reactivate. Talk to your pharmacist about setting up reminders if you’re on long-term therapy — adherence is the single strongest predictor of good outcomes.
Last medical review: April 2026. Next scheduled review: October 2026.
Authoritative references: WHO herpes simplex fact sheet · NHS genital herpes information · CDC genital herpes treatment guidelines · Corey L et al. Once-Daily Valacyclovir to Reduce the Risk of Transmission of Genital Herpes. N Engl J Med 2004;350:11-20.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.