







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
In five years, a class of drugs you had probably never heard of went from a diabetes medication to the most-prescribed weight-loss treatment in the developed world. Ozempic, Wegovy, Mounjaro, Zepbound — different brand names, overlapping molecules, competing head-to-head trials. Deciding between them has become one of the most common questions in obesity medicine.
This is a complete, evidence-based guide to GLP-1 weight loss injections and GIP/GLP-1 dual agonists for 2026. You’ll learn exactly what these drugs are, how the single-receptor GLP-1 agonists differ from the dual-agonist tirzepatide class, which one delivers more weight loss head-to-head, what the side-effect profile actually looks like, who should and shouldn’t start treatment, and how the upcoming triple-agonist retatrutide will reshape the landscape. No hype, no marketing — just the clinical science.
Key Takeaways
- GLP-1 mono-agonists (Ozempic, Wegovy, Rybelsus, Saxenda) produce 6-15% mean body weight reduction at ~68 weeks.
- GIP/GLP-1 dual-agonists (Mounjaro, Zepbound — both tirzepatide) produce 20-22% — the biggest single-drug effect ever seen in obesity medicine.
- Retatrutide (GIP + GLP-1 + glucagon triple-agonist, Phase 3 trials, approval expected 2026-27) is now producing up to 24% body weight loss.
- Mandatory 16-week dose titration is the single most important predictor of tolerability.
- Side effects are predominantly gastrointestinal — nausea, vomiting, constipation — and usually settle within 4-8 weeks at each dose.
- Weight tends to return once the drug is stopped; these are typically treated as long-term medications, not a “finish the course” plan.
Jump to a section
- What are weight loss injections?
- How they work (GLP-1 vs GIP/GLP-1)
- The drug family compared
- Weight loss efficacy head-to-head
- Dose titration schedule
- Side effects & safety
- Who is a candidate?
- How to start & stay on
- Lifestyle foundation
- Cost & access
- The triple-agonist era
- Frequently asked questions
- The bottom line
What Are Weight Loss Injections?
Quick Answer: What are GLP-1 weight loss injections?
GLP-1 weight loss injections are medications — typically once-weekly subcutaneous injections — that mimic natural gut hormones (incretins) to reduce appetite, slow digestion, and lower blood sugar. The newer class, GIP/GLP-1 dual-agonists like tirzepatide, activate two receptors and produce greater weight loss than GLP-1 alone. Most users lose 15-22% of body weight over 12-18 months when treatment is combined with lifestyle changes.
“Weight loss injections” is the everyday name for incretin-based therapies. Incretins are hormones naturally released from the gut when you eat — they signal satiety to the brain, slow stomach emptying, and nudge the pancreas to release insulin. The problem is that natural incretins get broken down within minutes. Modern weight-loss drugs are engineered analogues that last days.
The two most relevant incretins are GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide). The first generation of these drugs — liraglutide (Saxenda), semaglutide (Ozempic, Wegovy, Rybelsus) — targets GLP-1 only. The second generation — tirzepatide (Mounjaro, Zepbound) — activates both GLP-1 and GIP receptors. A third generation is in late-stage trials: retatrutide targets GLP-1, GIP, and glucagon receptors simultaneously.
All of these work because obesity is, at its core, a disorder of hunger signalling. When incretins are boosted, hunger drops, satiety rises, and food intake falls — almost always voluntarily, without the white-knuckled effort that purely behavioural calorie restriction demands.
How GLP-1 and GIP/GLP-1 Injections Actually Work
The four GLP-1 actions
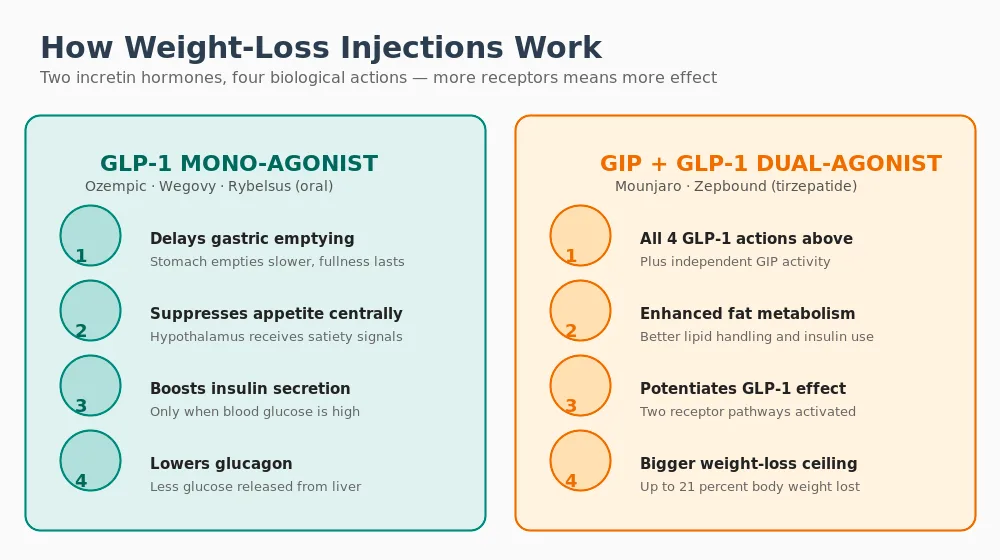
Every GLP-1 agonist — whether semaglutide, liraglutide, or the GLP-1 arm of tirzepatide — produces four linked effects:
- Delayed gastric emptying. Food leaves the stomach more slowly, so fullness lasts for hours longer after a meal.
- Central appetite suppression. GLP-1 crosses into the hypothalamus and activates satiety neurons, dampening hunger and food-related thoughts.
- Enhanced insulin secretion (glucose-dependent). The pancreas releases more insulin only when blood glucose is elevated, reducing post-meal glucose spikes without causing hypoglycaemia.
- Reduced glucagon. Less glucose is released from the liver, improving baseline glucose control.
Together, these effects produce spontaneous calorie reduction of 300-700 kcal/day in most users. Patients routinely describe eating half their previous portion and feeling done, or forgetting to eat altogether — what researchers call the reduction of “food noise.”
Why adding GIP makes it better
GIP is a complementary incretin released primarily in response to fat and carbohydrate ingestion. Activating the GIP receptor:
- Potentiates the central appetite-suppressing effect of GLP-1
- Improves insulin sensitivity in adipose tissue
- Enhances fat cell differentiation and lipid storage efficiency — counterintuitive but clinically produces better body-composition outcomes
- Appears to reduce the nausea threshold at any given level of weight loss, improving tolerability
The practical result: tirzepatide produces roughly 40% more weight loss than semaglutide at matched doses. For head-to-head data, see our in-depth Tirzepatide vs Semaglutide comparison.
The Weight-Loss Injection Family Compared
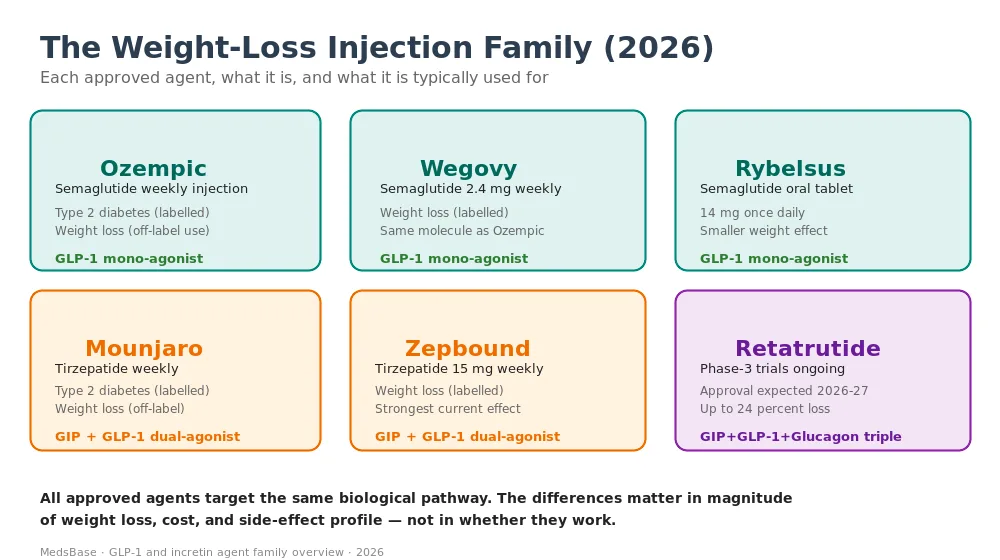
Ozempic (semaglutide, weekly injection)
FDA-approved for type-2 diabetes in 2017. Dosed 0.25 → 2.0 mg weekly. Technically used off-label for weight loss, although the results at 2.0 mg approach those of Wegovy. It is the name most people know — partly because it was the first GLP-1 to go viral on social media.
Wegovy (semaglutide, higher dose for weight loss)
Same molecule as Ozempic, approved specifically for chronic weight management at a higher target dose of 2.4 mg weekly. Labelled for adults with BMI ≥30, or BMI ≥27 with an obesity-related comorbidity. STEP-1 trial showed 14.9% body weight loss at 68 weeks.
Rybelsus (oral semaglutide)
A tablet version, taken daily on an empty stomach with a small sip of water, then a 30-minute fast. Peak dose 14 mg. Weight loss effect is smaller than injectable semaglutide (typically 3-5%) because oral bioavailability is low. Suits patients who refuse injections. See Rybelsus for weight loss for a full write-up.
Saxenda (liraglutide, daily injection)
An older daily GLP-1 that was the first to get weight-loss labelling (SCALE trial, 2015). About 6% mean weight loss at 1 year — modest by current standards. Mostly superseded by weekly options but still used where cost or formulary restrictions mandate it.
Mounjaro (tirzepatide, weekly injection)
FDA-approved for type-2 diabetes in 2022. The first GIP/GLP-1 dual-agonist. Weekly injection, escalated 2.5 → 15 mg over five months. Used off-label for weight loss at the same dose.
Zepbound (tirzepatide, higher-dose weight-loss labelling)
Same molecule as Mounjaro, labelled specifically for chronic weight management since 2023. Results at 15 mg: around 21% body weight loss at 72 weeks — currently the strongest approved effect.
Retatrutide (triple-agonist, Phase 3)
Activates GIP, GLP-1, and glucagon receptors simultaneously. The third receptor (glucagon) stimulates energy expenditure — boosting metabolic rate rather than only reducing intake. Phase-2 data show up to 24% weight loss at 48 weeks. FDA approval anticipated late 2026 or 2027. See our dedicated Retatrutide guide for full mechanism and trial detail.
Weight Loss Efficacy — Head-to-Head
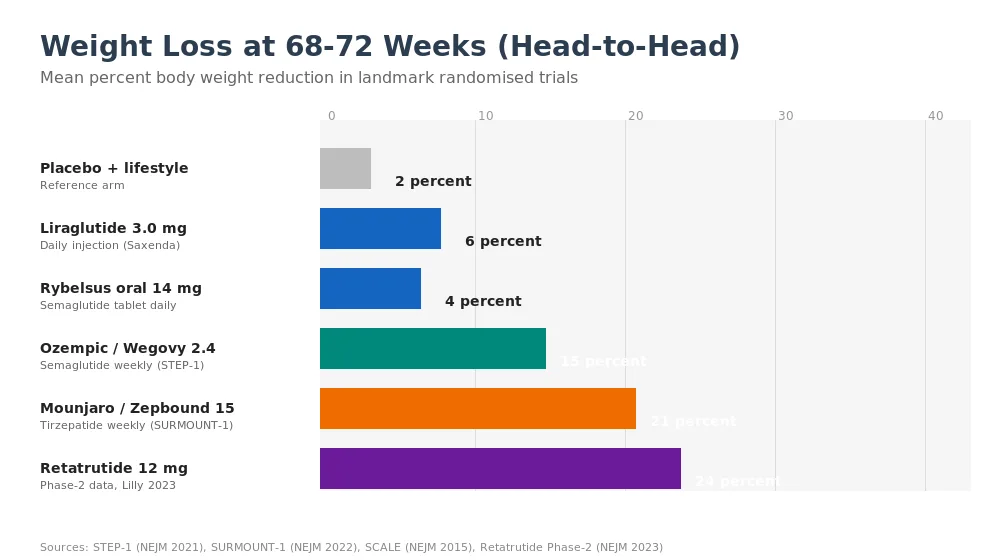
Research suggests — consistently across the SCALE, STEP, SURPASS, SURMOUNT, and Retatrutide programs — that weight-loss magnitude scales cleanly with receptor coverage.
| Agent | Class | Trial | Mean weight loss |
|---|---|---|---|
| Liraglutide 3.0 mg daily | GLP-1 | SCALE (NEJM 2015) | ~6% at 56 weeks |
| Rybelsus 14 mg oral | GLP-1 (oral) | PIONEER-4 / post-hoc | ~4% at 1 year |
| Semaglutide 2.4 mg weekly | GLP-1 | STEP-1 (NEJM 2021) | 14.9% at 68 weeks |
| Tirzepatide 15 mg weekly | GIP/GLP-1 dual | SURMOUNT-1 (NEJM 2022) | 20.9% at 72 weeks |
| Tirzepatide head-to-head vs semaglutide | GIP/GLP-1 dual | SURMOUNT-5 (2024) | 20.2% vs 13.7% — a 47% relative advantage |
| Retatrutide 12 mg weekly | GIP + GLP-1 + glucagon triple | NEJM 2023 Phase-2 | 24.2% at 48 weeks |
Early studies indicate the weight-loss effect continues to grow through at least 72 weeks for tirzepatide, and still hadn’t plateaued at 48 weeks for retatrutide — suggesting ultimate ceilings even higher than reported. For most individuals starting treatment today, 12-24% body weight loss over 12-18 months is a realistic planning figure depending on the drug chosen and dose achieved.
Dose Titration — The Most Important Part of Starting
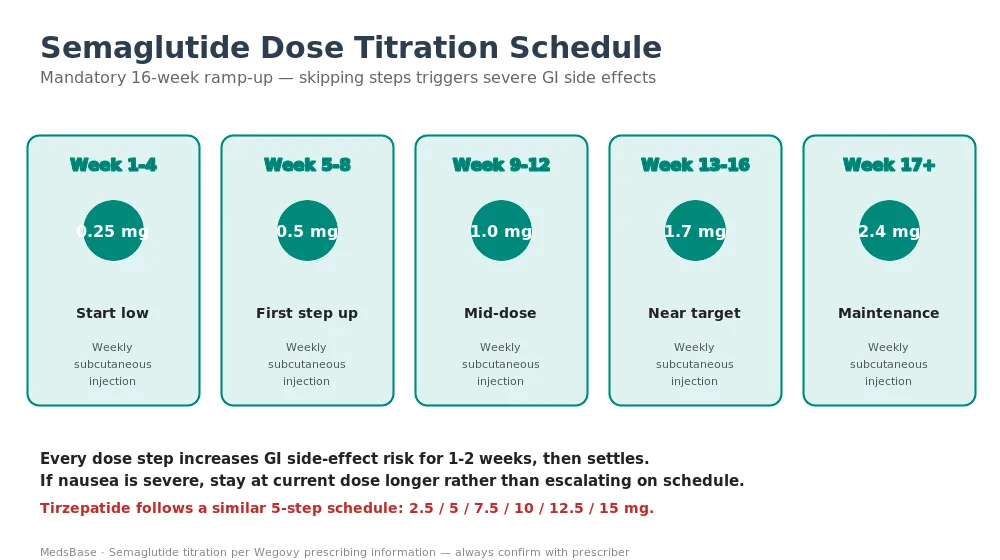
Every GLP-1 weight-loss drug uses a stepped dose-escalation protocol. This is not a product design quirk — it is the single most important determinant of whether someone stays on the drug.
Semaglutide (Wegovy) titration:
- Weeks 1-4: 0.25 mg weekly
- Weeks 5-8: 0.5 mg weekly
- Weeks 9-12: 1.0 mg weekly
- Weeks 13-16: 1.7 mg weekly
- Week 17+: 2.4 mg weekly (maintenance target)
Tirzepatide (Zepbound / Mounjaro) titration:
- Weeks 1-4: 2.5 mg weekly
- Weeks 5-8: 5.0 mg weekly
- Weeks 9-12: 7.5 mg weekly
- Weeks 13-16: 10 mg weekly
- Weeks 17-20: 12.5 mg weekly
- Week 21+: 15 mg weekly (target for weight management)
Each step increases the risk of nausea, vomiting, and constipation for 1-2 weeks before settling. If side effects are severe, stay longer at the current dose rather than escalating on schedule. Prescribers routinely hold patients at a sub-maximal dose indefinitely if that dose produces adequate weight loss and acceptable tolerability.
Side Effects and Safety
| Side effect | Frequency | Severity / management |
|---|---|---|
| Nausea | 40-50% first 8 weeks | Mild-moderate, resolves with slow titration |
| Constipation | 20-25% | Increase fluid + fibre; magnesium citrate if needed |
| Vomiting | 10-20% | Hold dose; small frequent meals |
| Diarrhoea | 10-15% | Mild; temporary |
| Injection-site reaction | 5-10% | Rotate sites; mild erythema |
| Gallbladder issues | 1-2% | Cholelithiasis; rapid weight loss is the trigger |
| Pancreatitis | <0.5% | Rare; stop drug if suspected |
| Muscle mass loss | Variable | Mitigate with protein + resistance training |
| “Ozempic face” | Cosmetic | Facial fat loss with any significant weight reduction |
The black-box warning on all GLP-1 and dual-agonist agents is a theoretical risk of medullary thyroid carcinoma (MTC) based on rodent studies. The link in humans has not been confirmed in 10+ years of post-marketing data, but the FDA mandates contraindication in patients with personal or family history of MTC or MEN2 syndrome. For context on the facial cosmetic effect, see “Ozempic face” — what it is and how to avoid it.
Who Is a Candidate for GLP-1 Injections?
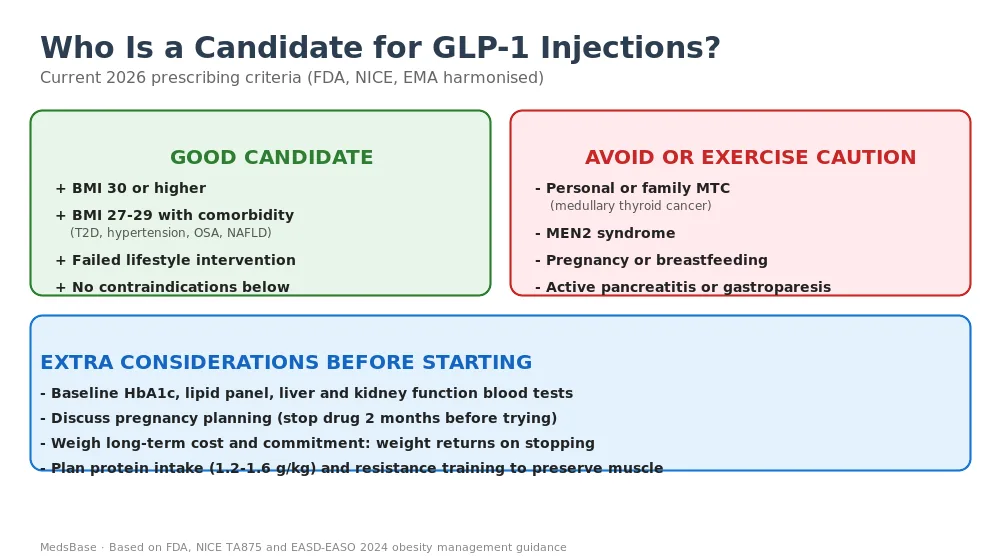
Ideal candidates
- Adults with BMI ≥30 (obesity)
- Adults with BMI 27-29 with at least one weight-related comorbidity (type-2 diabetes, hypertension, dyslipidaemia, obstructive sleep apnoea, non-alcoholic fatty liver disease)
- Have already attempted ≥6 months of structured lifestyle intervention without sufficient result
- No contraindications (see below)
- Willing to commit to long-term use — weight tends to return on stopping
Contraindications
- Personal or family history of medullary thyroid carcinoma (MTC)
- Multiple Endocrine Neoplasia type 2 (MEN2) syndrome
- Pregnancy or active family planning — stop the drug at least 2 months before attempting pregnancy
- Active pancreatitis or known severe gastroparesis
- Hypersensitivity to semaglutide, tirzepatide, or excipients
How to Start — Practical Guidance
- Get a baseline clinical assessment. Weight, height, BMI, blood pressure, HbA1c, lipid profile, liver and kidney function tests, plus thyroid review if MTC concerns exist.
- Discuss pregnancy planning with all patients of reproductive potential.
- Choose the agent based on budget, injection preference, and weight-loss target. For most patients tirzepatide (Zepbound / Mounjaro) is first-choice when available; semaglutide (Wegovy / Ozempic) remains a reasonable alternative.
- Follow the titration schedule religiously. Resist the urge to push the dose if side effects are settling — weight loss builds over months, not weeks.
- Plan your nutrition. Reduced appetite can lead to protein under-intake and muscle mass loss. Target 1.2-1.6 g protein per kg body weight per day. Add resistance training 2-3 times weekly.
- Stay hydrated. 2-3 L of fluid daily helps prevent constipation and blunts nausea.
- Reassess every 3 months. Weight, blood pressure, HbA1c, lipid response, side-effect burden. Continue as long as benefit outweighs cost and tolerability.
Browse our weight loss medication range at MedsBase, or read companion guides: how to get Ozempic for weight loss, peptide stacks for fat loss, and Rybelsus for weight loss.
Lifestyle Is Still the Foundation
GLP-1 and dual-agonist injections are powerful — but they are not a replacement for the underlying habits that determine long-term outcome. Patients who combine the injection with deliberate nutrition and exercise changes lose more weight, preserve more muscle, feel better during treatment, and hold onto their results longer when the drug dose is eventually reduced or paused.
Protein target
The appetite-suppressing effect of GLP-1 drugs often leads to under-eating protein in particular — because protein-rich meals produce the longest satiety signals even at smaller portions. Aim for 1.2-1.6 g protein per kg body weight per day. For a 90 kg adult that’s 108-144 g daily — typically from lean meat, fish, eggs, Greek yogurt, cottage cheese, tofu, and a daily whey or soy protein shake if food intake has fallen.
Resistance training
Two to three sessions per week of progressive resistance training preserves lean mass during weight loss. Compound movements (squats, deadlifts, press, row) are more efficient than isolation work. Even bodyweight training (push-ups, bodyweight squats, resistance-band rows) works for beginners. The goal is not muscle gain — it is loss prevention, which is easier to achieve.
Cardiovascular exercise
150 minutes per week of moderate aerobic activity (brisk walking, cycling, swimming, elliptical) improves insulin sensitivity, supports cardiovascular health, and modestly increases total energy expenditure. More is better up to around 300 minutes weekly; beyond that, diminishing returns.
Hydration and fibre
Constipation is the second-most-common side effect of GLP-1 injections. Drink 2-3 litres of fluid daily and target 25-35 g of dietary fibre from vegetables, legumes, whole grains, and fruit. If constipation persists despite this, magnesium citrate or a bulk-forming laxative (psyllium) is well tolerated.
Sleep and stress
Chronic poor sleep and chronically elevated cortisol both undermine weight-loss results by raising appetite, reducing activity, and impairing glucose control. Prioritising 7-8 hours of good-quality sleep amplifies every other intervention. Stress-management practices — regular exercise, mindfulness, therapy for chronic stressors — play similar roles.
The simple test: at one year on treatment, the patients who walk, strength train, and eat adequate protein consistently look and feel dramatically different from the patients who relied on the injection alone — even when both groups have lost similar absolute weight on the scale.
Cost and Access
Costs for branded Wegovy, Ozempic, Mounjaro, and Zepbound in Western markets typically run $900-1,500 per month without insurance. With insurance coverage varying wildly by plan and country, out-of-pocket ranges from $25 to full sticker price. Generic semaglutide will not be available in the US until at least 2031 under current patent protection.
Compounded semaglutide (dispensed by compounding pharmacies during drug shortages) has been widely available at lower cost in the US in 2024-25 but is under increasing FDA scrutiny. Outside the US, generic tirzepatide and semaglutide formulations are available in some markets.
The long-term commitment is real. If the drug is priced at $800/month and you plan to stay on it for 5 years, that’s $48,000 — comparable to bariatric surgery in total cost, but spread over time rather than paid upfront.
The Triple-Agonist Era
Retatrutide is the first in a new class of triple-agonist drugs that add glucagon receptor activity to the GIP/GLP-1 combination. Glucagon raises energy expenditure — so instead of producing weight loss only by reducing intake, retatrutide also modestly increases metabolic rate.
Phase-2 data (NEJM 2023) showed:
- 12 mg weekly: 24.2% body weight loss at 48 weeks (still on trajectory)
- Tolerability broadly similar to tirzepatide
- Substantial improvements in liver fat, cardiovascular risk markers, and glucose metrics
Phase-3 trials are running through 2026. Regulatory approval is anticipated in late 2026 or 2027. Ongoing research is also exploring amylin analogs (cagrilintide — pemvidutide) as combination partners; the amylin + GLP-1 combination (CagriSema) has produced early data rivalling tirzepatide.
What this means practically: the 2026-2028 period is likely to see a step-change in available weight-loss pharmacotherapy, potentially moving the field from 20% to 25-30% weight loss as a routine expectation.
Beyond raw weight loss, the next wave of these drugs is being studied for a wider range of conditions: cardiovascular outcome reduction (SELECT showed semaglutide cut major adverse cardiovascular events by 20% in people without diabetes), chronic kidney disease progression, non-alcoholic steatohepatitis (NASH), sleep apnoea severity, and even early Alzheimer’s disease. Several of these indications are already producing positive Phase-3 data and may expand the label criteria significantly over the next few years.
Frequently Asked Questions
What’s the difference between Ozempic and Wegovy?
Same molecule (semaglutide), different FDA labelling and typical dose. Ozempic is approved for type-2 diabetes at doses up to 2.0 mg weekly. Wegovy is approved for chronic weight management at a maximum of 2.4 mg weekly. Weight loss results at Ozempic’s 2.0 mg come close to Wegovy’s 2.4 mg, so off-label use of Ozempic for weight loss is common — but it isn’t its licensed indication.
Is tirzepatide better than semaglutide for weight loss?
For most people, yes — head-to-head in SURMOUNT-5 (2024), tirzepatide 15 mg produced 20.2% weight loss versus 13.7% for semaglutide 2.4 mg, a 47% relative advantage. Tirzepatide is also often better tolerated at matched weight-loss levels, because the GIP component appears to reduce nausea. Semaglutide remains a sensible choice when cost, insurance coverage, or supply favours it.
What happens if I stop taking a GLP-1 injection?
Most people regain two-thirds of the lost weight within 12 months of stopping, per the STEP-4 withdrawal study. Appetite, gastric emptying, and incretin activity all return to pre-treatment baseline. This is why obesity medicine now treats GLP-1 injections as long-term medication — more like blood-pressure or cholesterol drugs than a finite course.
Do GLP-1 injections cause muscle loss?
Some, yes — about 25-40% of lost weight can be lean mass if no action is taken. The mitigation is deliberate: target 1.2-1.6 g protein per kg body weight daily, resistance-train 2-3 times per week, and prioritise slow-release protein sources. Trials with structured exercise programmes show most users preserve lean mass within normal ranges.
Can I get GLP-1 injections without diabetes or obesity?
Not through proper medical channels. Prescribing outside the licensed BMI thresholds (BMI ≥30, or ≥27 with comorbidity) falls outside formal guideline support. Off-label prescribing for cosmetic weight loss at normal BMI exists but is ethically and clinically controversial — the safety data is thin and the cost-benefit poor for people not clinically obese.
Are GLP-1 injections safe long-term?
Current evidence (up to 10 years for older GLP-1s, 5 years for semaglutide, 3-4 years for tirzepatide) shows a reassuring safety profile with no unexpected long-term signals. Cardiovascular outcome trials (SUSTAIN-6, SELECT, LEADER) have actually shown reductions in major cardiovascular events. The longest-term questions — bone density effects over decades, cancer signals — won’t be fully answered until the 2030s.
Will GLP-1 injections get cheaper?
Branded prices in the US are unlikely to fall substantially before patent expiry (semaglutide: 2031; tirzepatide: 2036). In the meantime, competition from compounded formulations, retatrutide entering the market, and potential alternatives like oral orforglipron may pressure pricing. Outside the US, generic semaglutide is already available in several markets at 10-30% of the branded price.
Can I drink alcohol on a GLP-1 injection?
Many users find their desire for alcohol drops dramatically — part of the “food noise” reduction appears to apply to alcohol cravings too. Ongoing research is exploring GLP-1 drugs as treatments for alcohol use disorder. Modest drinking is not contraindicated, but heavy drinking compounds GI side effects and is discouraged on safety and tolerability grounds.
The Bottom Line
GLP-1 weight loss injections represent the biggest therapeutic advance in obesity medicine in 50 years. Semaglutide delivers 15% weight loss on average. Tirzepatide delivers 21%. Retatrutide, already in late-stage trials, is reaching 24% and rising. Combined with the right lifestyle foundation, these drugs now put goals that used to require bariatric surgery into the reach of a weekly self-administered injection.
The playbook for 2026: confirm you meet the criteria, get a proper baseline workup, pick the most potent agent your budget and access allow, titrate patiently over 16-20 weeks, build a nutrition and resistance-training routine around it, and plan for long-term use. The drugs work; the hard part is the commitment.
Browse our full weight loss medication catalogue at MedsBase. For related reading, see our Tirzepatide vs Semaglutide comparison, Retatrutide triple-agonist guide, and peptide stacks for fat loss.
⚕️ Medical Disclaimer. This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Semaglutide, tirzepatide, liraglutide and retatrutide are prescription medications requiring evaluation by a qualified healthcare professional. Never start, stop, or combine GLP-1 agonist therapies without speaking to your doctor, particularly if you are pregnant, planning pregnancy, breastfeeding, or have a personal or family history of medullary thyroid cancer, MEN2 syndrome, or pancreatitis. Always follow the prescribing clinician’s guidance.
Last updated: 2026-04-17 · Reviewed by MedsBase Clinical Content Team.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.