







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Medically reviewed by the MedsBase Editorial Team · Last updated: 18 April 2026
Around one in six adults aged 14 to 49 worldwide lives with genital HSV-2, and more than two-thirds of all adults under 50 carry oral HSV-1, according to the World Health Organization. For most of them, outbreaks are manageable — but the question of how to manage them splits almost perfectly down the middle: take an antiviral every day, or only when an outbreak starts?
This guide walks through the evidence on daily vs episodic herpes antiviral treatment, compares the three main drugs used in both strategies, and shows exactly when each approach delivers the best results. You will learn who benefits most from each regimen, what the landmark randomised trials show, how transmission risk changes with suppressive therapy, and how to discuss a switch with your clinician.
Key Takeaways
- Daily suppressive therapy reduces outbreak frequency by roughly 70–80% and cuts HSV-2 transmission to a partner by about 48%.
- Episodic therapy shortens each outbreak by 1–2 days when started at the first prodrome but does not reduce annual recurrence rate.
- Six or more outbreaks a year is the common guideline threshold to consider daily therapy.
- Valacyclovir, acyclovir, and famciclovir are all effective; choice usually depends on dosing convenience and cost.
- Suppressive courses are typically reviewed at 12 months to reassess natural outbreak frequency.
Jump to a Section
Herpes Antivirals: Daily vs Episodic Treatment — Which Works Best for You?
What Are Herpes Antivirals? (Definition & Background)
Herpes antivirals are prescription nucleoside analogue medications — chiefly acyclovir, valacyclovir, and famciclovir — that block replication of the herpes simplex virus. Taken daily they suppress outbreaks before they start; taken episodically they shorten an outbreak already in progress.
Herpes simplex is a lifelong infection. After the initial outbreak, the virus retreats up the sensory nerves and settles in the ganglia, where it stays quiet until a trigger — stress, UV exposure, fever, hormonal shifts, or immune suppression — reactivates it. Antivirals cannot clear the virus from the ganglia, but they can sharply cut how often and how severely it emerges.
Three drugs dominate clinical practice worldwide:
- Acyclovir (the original 1980s molecule) — effective but requires 2–5 doses per day due to short half-life.
- Valacyclovir — an acyclovir prodrug with roughly 3× the oral bioavailability, allowing once- or twice-daily dosing.
- Famciclovir — a penciclovir prodrug, similar convenience to valacyclovir, often used in herpes zoster as well.
All three share a mechanism of action that is uniquely selective for herpes-infected cells, which is why they carry a genuinely favourable long-term safety profile even on multi-year daily dosing. For a deeper drug-by-drug breakdown, see our valacyclovir vs acyclovir comparison.
How Do Herpes Antivirals Work? (Mechanism & Science)
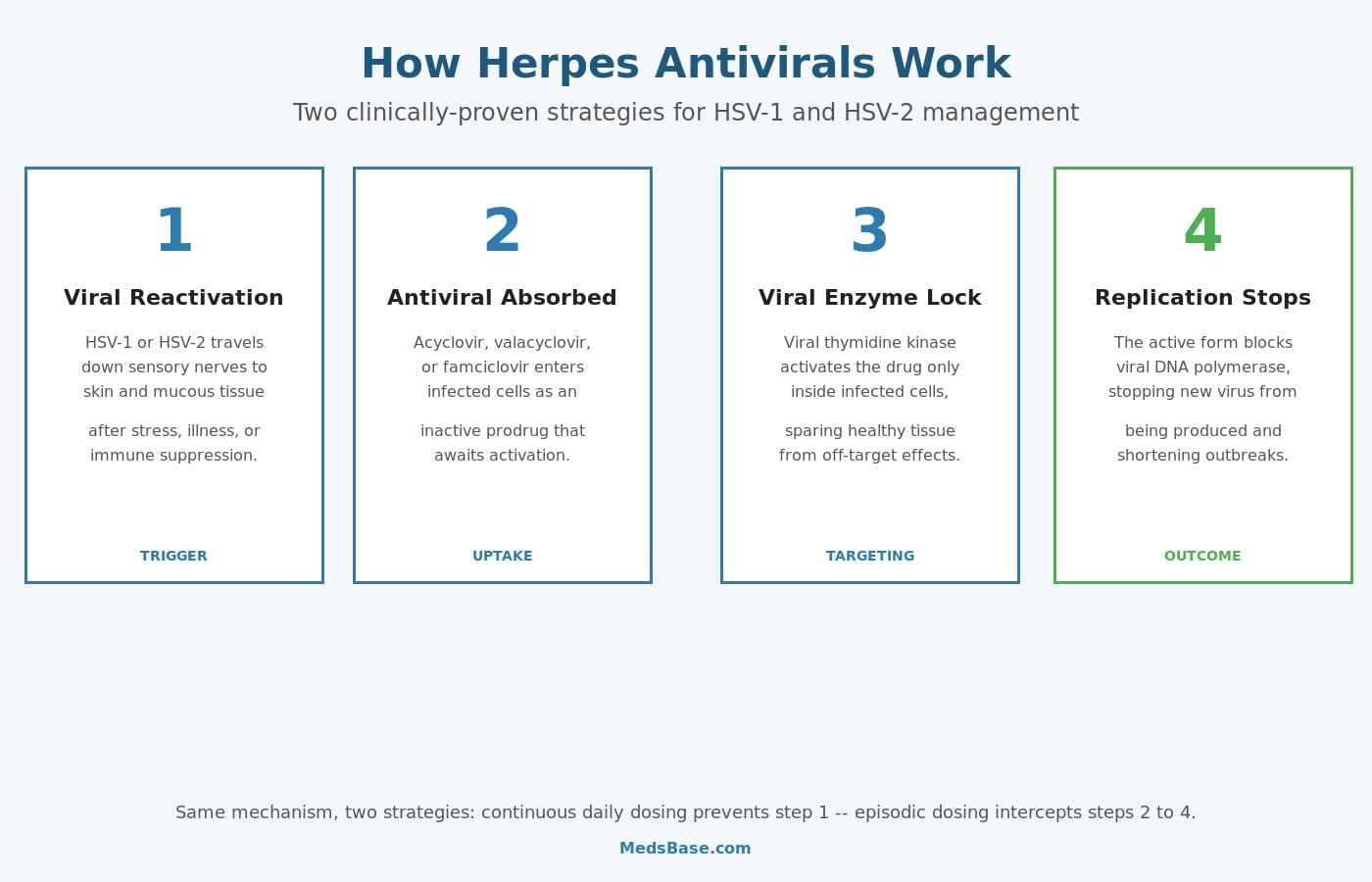
Herpes antivirals are prodrugs — inactive until they reach an infected cell. That is the clever part of their design.
When HSV reactivates, it produces its own enzyme called viral thymidine kinase. Acyclovir (and its prodrug cousins) looks structurally similar to a natural building block of DNA, so the viral enzyme latches onto it and adds a phosphate group. Human cellular enzymes do this poorly — they largely ignore the drug. This means the active form of the medicine accumulates almost exclusively inside infected cells, which is why these drugs spare healthy tissue and produce so few side effects relative to their potency.
Once activated, the phosphorylated drug competes with the normal DNA building block (guanosine triphosphate) for the viral DNA polymerase. When the polymerase grabs it, new viral DNA synthesis grinds to a halt and the outbreak is capped.
The mechanism is identical whether you take the drug daily or episodically — only the timing changes. Daily dosing keeps drug concentrations high enough to shut down reactivation before the virus can generate visible lesions. Episodic dosing catches an outbreak in its earliest stage, when virus is replicating rapidly but lesions have not yet formed, and cuts it short.
Key Uses & Applications — Who Needs Daily vs Episodic?
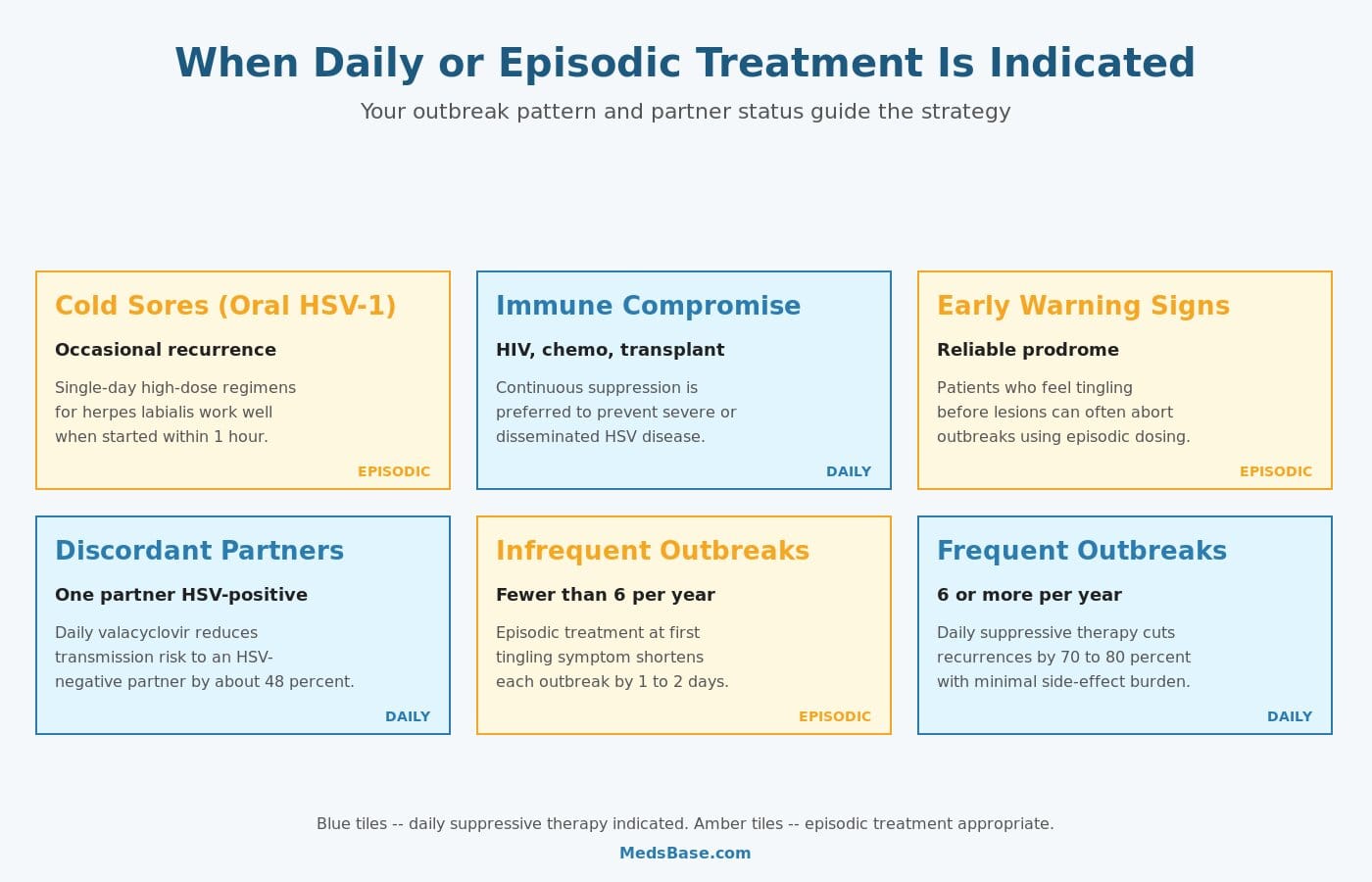
1. Frequent Outbreaks (Six or More Per Year)
This is the textbook indication for daily suppressive therapy. The US Centers for Disease Control, the UK BASHH guidelines, and the International Union against Sexually Transmitted Infections all agree: once outbreaks reach six or more a year, suppression outperforms episodic treatment on every metric that matters — fewer outbreaks, shorter outbreaks when they do occur, less shedding, better quality of life.
2. Infrequent Outbreaks with a Reliable Prodrome
If you only get an outbreak once or twice a year and you reliably notice the early tingling sensation 12–24 hours before lesions appear, episodic therapy is often the better fit. A single-day or 3-day high-dose course started at the prodrome can abort the outbreak entirely in 30–50% of cases, and shorten it by 1–2 days in the rest.
3. Discordant Sexual Partnerships
When one partner has HSV-2 and the other does not, daily valacyclovir is the only medication shown in a randomised controlled trial to reduce transmission. This is a strong argument for suppression even in people whose personal outbreak burden is low — you are treating transmission risk, not just symptoms.
4. Immunocompromised Patients
People with HIV, those on chemotherapy, organ-transplant recipients, and patients on long-term high-dose steroids are at risk of atypical, prolonged, or disseminated herpes. Continuous suppressive therapy is usually preferred at higher doses (e.g. acyclovir 400–800 mg twice daily) and reviewed regularly by the treating specialist.
5. Recurrent Cold Sores (Oral HSV-1)
Most people with oral cold sores manage with episodic therapy. One-day high-dose valacyclovir (2 g twice in a day) or famciclovir (1.5 g single dose) started within the first hour of symptoms can dramatically shorten the outbreak. Daily suppression is reserved for people with monthly or more frequent cold sores, or whose outbreaks trigger erythema multiforme.
6. Pregnancy (Late-Third-Trimester Suppression)
Current obstetric guidance recommends daily suppression from 36 weeks in pregnant women with a history of genital HSV, to reduce the likelihood of an outbreak at delivery and therefore the need for caesarean section. This is a short, defined course rather than indefinite suppression.
Safety Profile, Side Effects & Dosage
All three core antivirals have been in wide clinical use for 25–40 years. Acyclovir has been taken safely by people on continuous daily suppression for more than 20 years in follow-up cohorts, with no signal of cumulative organ toxicity.
The most common adverse effects are mild and transient. The table below summarises what to expect.
| Side Effect | Frequency | Severity |
|---|---|---|
| Headache | Common (13–38%) | Usually mild |
| Nausea | Common (5–15%) | Mild, improves with food |
| Abdominal pain | Uncommon (<5%) | Mild |
| Dizziness / fatigue | Uncommon (2–6%) | Mild |
| Rash | Rare (<1%) | Usually mild — stop and review if widespread |
| Reversible rise in creatinine | Rare — dehydration or high IV doses | Moderate — hydrate well, adjust dose |
| Neurotoxicity (confusion, tremor) | Very rare — impaired kidneys / very high doses | Serious — seek urgent review |
Typical oral dosing in adults with normal renal function:
- Daily suppression: valacyclovir 500 mg once daily (or 1 g once daily for ≥10 outbreaks/year), acyclovir 400 mg twice daily, or famciclovir 250 mg twice daily.
- Episodic genital outbreak: valacyclovir 500 mg twice daily for 3 days, acyclovir 800 mg three times daily for 2 days, or famciclovir 1 g twice in one day.
- Episodic cold sore: valacyclovir 2 g twice in a single day, or famciclovir 1.5 g single dose.
Dose reduction is mandatory in moderate-to-severe renal impairment. Adequate hydration is important for anyone on higher doses or with borderline kidney function.
Special Considerations by Life Stage and Health Status
Pregnancy. Acyclovir and valacyclovir have decades of post-marketing safety data in pregnancy and are widely used from 36 weeks gestation in women with a history of genital HSV, to reduce the probability of an outbreak at delivery and therefore of caesarean section. Famciclovir has less pregnancy data and is typically reserved for cases where the other two are not tolerated.
Breastfeeding. Acyclovir and valacyclovir appear in breast milk in small amounts but have not been associated with infant harm, and both are considered compatible with breastfeeding by the American Academy of Pediatrics and UK NICE guidance.
Kidney disease. Dose intervals are lengthened in proportion to creatinine clearance. Mild renal impairment typically needs no change; moderate impairment (eGFR 30–50) drops daily suppression to every 24–48 hours; severe impairment requires specialist input. Neurotoxicity is almost always a dosing-error signal in someone with unrecognised kidney disease.
Older adults. Age itself is not a contraindication, but eGFR naturally falls with age, so baseline renal function should be checked before starting suppressive therapy in anyone over 65. Adequate fluid intake matters more in this group.
Travel. Time-zone shifts can derail daily dosing briefly, but a missed dose or two is not clinically dangerous — simply resume the normal schedule on arrival. For episodic therapy, carry a course in your hand luggage so you can start treatment immediately if a prodrome appears while away from your usual medicine cabinet.
What Does the Research Say?
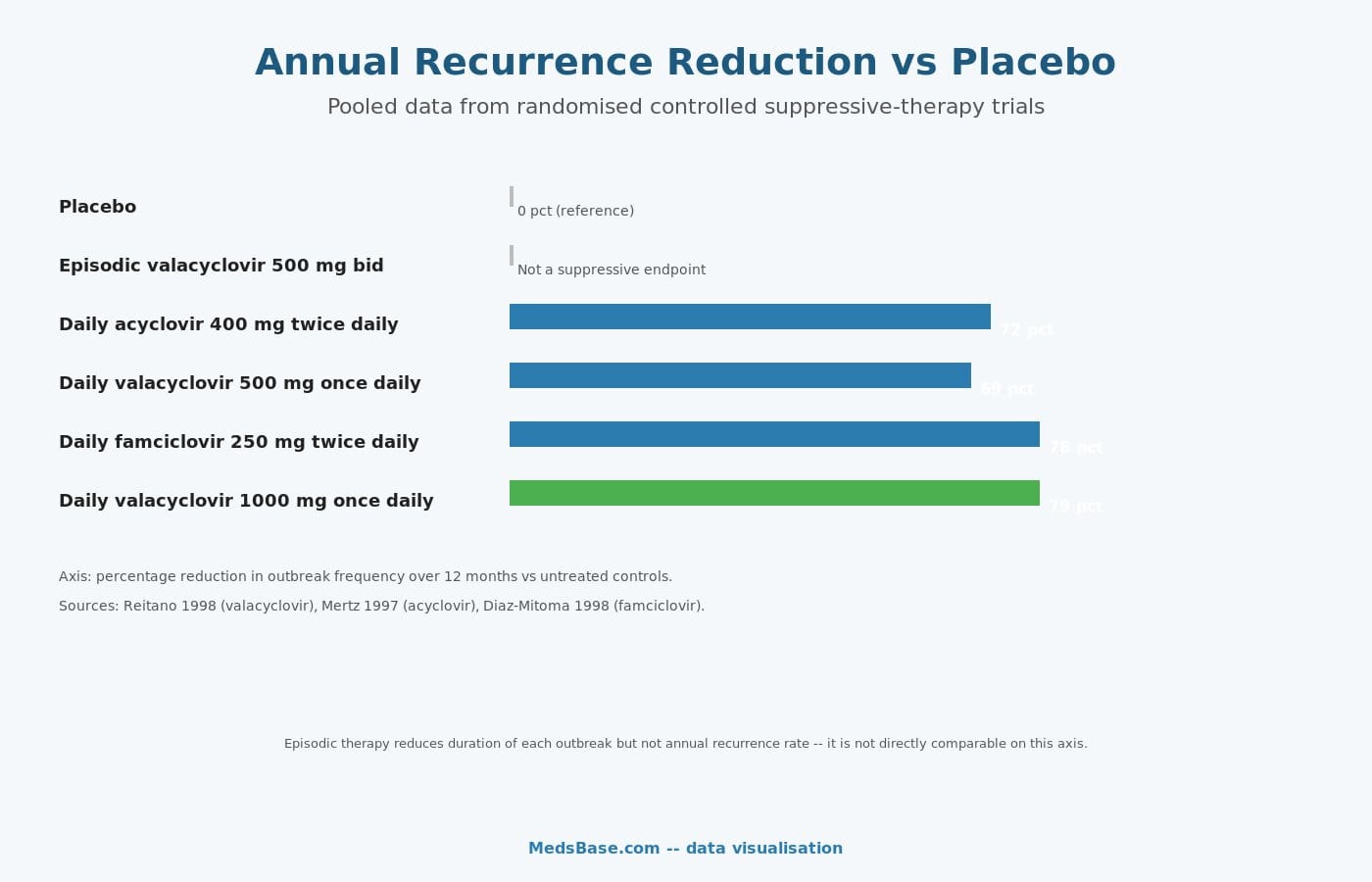
Four trials anchor the modern evidence base. The pooled results show a remarkably consistent picture.
| Study | Year | Finding | Source |
|---|---|---|---|
| Reitano et al. — Valacyclovir dose-ranging trial | 1998 | Valacyclovir 500 mg once daily reduced recurrences by 69%; 1 g once daily by 79%. | J Infect Dis |
| Mertz et al. — Long-term acyclovir suppression | 1997 | Acyclovir 400 mg twice daily cut recurrences by about 72% over 5 years, with stable safety. | Arch Intern Med |
| Diaz-Mitoma et al. — Famciclovir suppression | 1998 | Famciclovir 250 mg twice daily prevented an outbreak in 78% of treated participants over 12 months. | JAMA |
| Corey et al. — Valacyclovir for transmission reduction | 2004 | Daily valacyclovir 500 mg reduced HSV-2 transmission to susceptible partners by 48% over 8 months. | N Engl J Med |
Across the suppressive trials, research suggests a ceiling effect around the 75–80% recurrence-reduction mark — pushing doses higher appears to buy little extra benefit. What daily therapy does uniquely well, beyond outbreak reduction, is reduce asymptomatic viral shedding. Corey’s 2004 trial showed that even though lesion-day reductions were dramatic, most of the transmission-prevention effect came from suppressing the silent shedding that happens between outbreaks.
Episodic therapy sits in a different evaluation universe. Its endpoint is not annual recurrence rate (it does not change that) but outbreak duration and severity. Pivotal episodic trials in the late 1990s and early 2000s consistently showed 1–2 days off the average outbreak duration and 1–2 fewer days of pain, with the largest benefit when treatment was initiated within 6 hours of prodrome onset.
Recognising Your Prodrome — the Key to Successful Episodic Therapy
Episodic treatment lives or dies on timing, and timing depends on recognising your own prodrome. About 50–75% of people with recurrent HSV-2 report some form of prodromal warning — most commonly a tingling, itching, burning, or mild nerve-pain sensation in the area where lesions later appear. Some describe it as a “knowing” — a familiar feeling that precedes every outbreak by 12–24 hours.
If you are new to herpes or unsure whether you have a prodrome, keep a simple log for three outbreaks: what sensation did you notice in the 24 hours before a lesion appeared, and where on the body? Patterns usually emerge quickly. People with a reliable prodrome are the ideal candidates for episodic therapy because they can intercept viral replication at its peak and often abort the outbreak entirely.
Those without a prodrome — roughly a quarter of people with recurrent HSV — still benefit from episodic therapy, but the outbreak is usually already underway by the time treatment starts, so benefit is smaller (about one day shortening rather than two). This group often does better on daily suppression.
Daily vs Episodic — Side-by-Side Comparison
Both strategies use the same drugs. The difference is timing, pill burden, and what outcomes they optimise for.
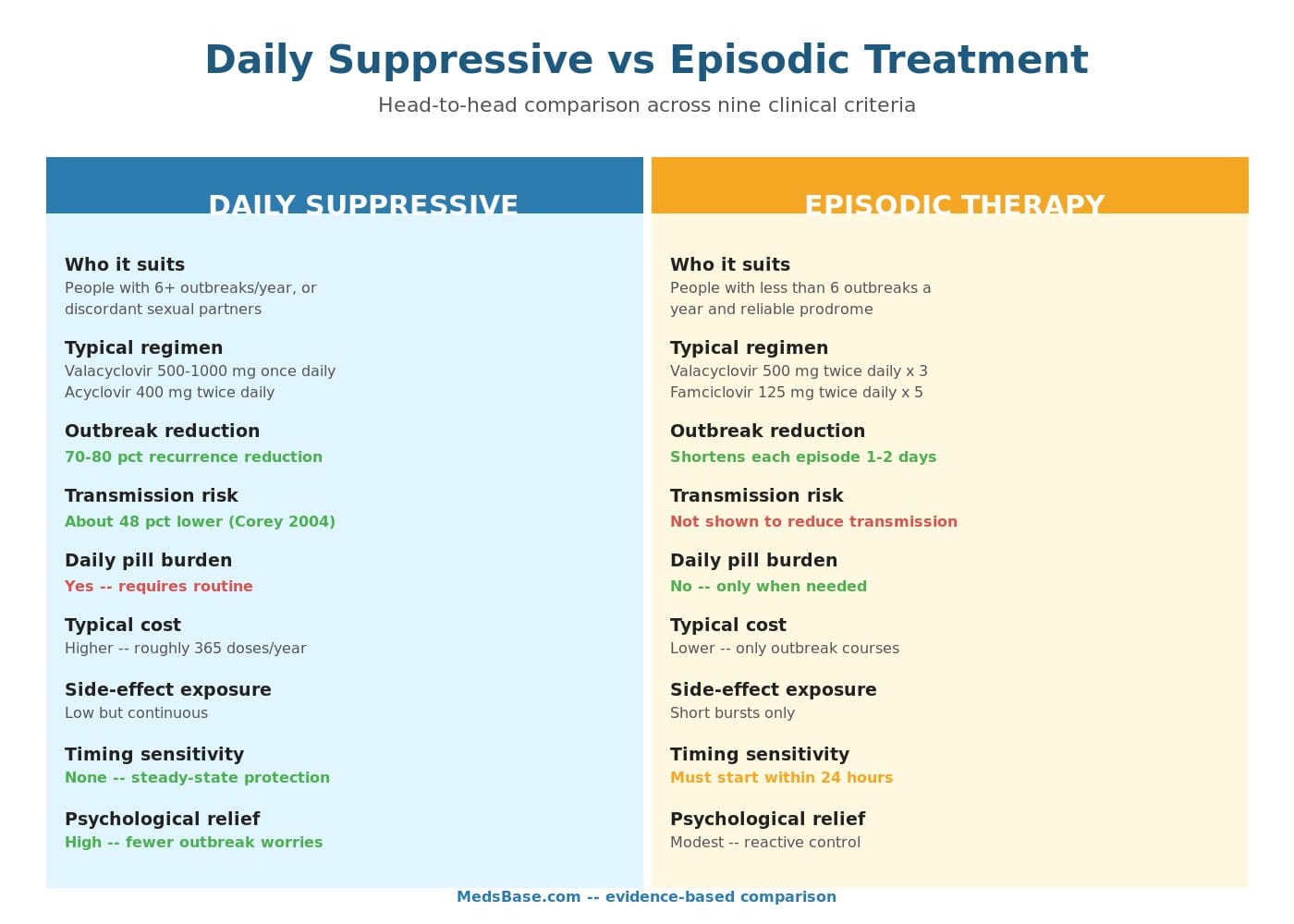
| Criterion | Daily Suppressive | Episodic |
|---|---|---|
| Best for | ≥6 outbreaks/year, discordant partners, immune suppression | <6 outbreaks/year, reliable prodrome |
| Typical regimen | Valacyclovir 500 mg once daily | Valacyclovir 500 mg twice daily × 3 days |
| Primary endpoint | 70–80% fewer outbreaks per year | 1–2 days shorter per outbreak |
| Transmission reduction | ~48% reduction (Corey 2004) | Not demonstrated |
| Daily pill burden | Yes — indefinite | No — only during outbreaks |
| Cost impact | Higher annualised cost (~365 doses/year) | Lower — only short courses |
| Side-effect exposure | Low but continuous | Short bursts only |
| Timing sensitivity | None — steady-state protection | Must start within 24 hours of prodrome |
| Psychological benefit | High — fewer outbreak worries | Modest — reactive |
| Review cadence | At 12 months — trial break recommended | As outbreaks change |
A common middle-ground approach is to start with 12 months of daily suppression, attempt a structured break to reassess natural outbreak frequency, and then transition to either continued suppression or episodic therapy based on what the follow-up data shows.
Common Mistakes Patients Make with Each Strategy
On daily suppression, the biggest mistake is inconsistent dosing. The drugs work by maintaining a steady-state blood level; dropping below the threshold for even a few days opens the door to reactivation. If remembering a daily pill is genuinely difficult, a once-daily valacyclovir regimen is usually easier to stick with than twice-daily acyclovir. Pair it with an existing habit — morning coffee, teeth-brushing, bedtime — rather than a standalone alarm, and adherence typically rises.
On episodic therapy, the biggest mistake is starting too late. People who wait until a lesion appears to fill a prescription miss the window where antivirals actually do their most useful work. The fix is to hold a standby supply at home — most clinicians will write a prescription for several pre-emptive courses so you can self-start treatment the moment a prodrome arrives. Make sure the supply does not expire between outbreaks.
A subtler mistake on both strategies is not reviewing. Herpes recurrence patterns evolve over years — what looked like ten outbreaks a year in your late 20s may be two a year in your late 30s. Annual review with a clinician catches these transitions and matches the strategy to your current biology, not the pattern you had three years ago.
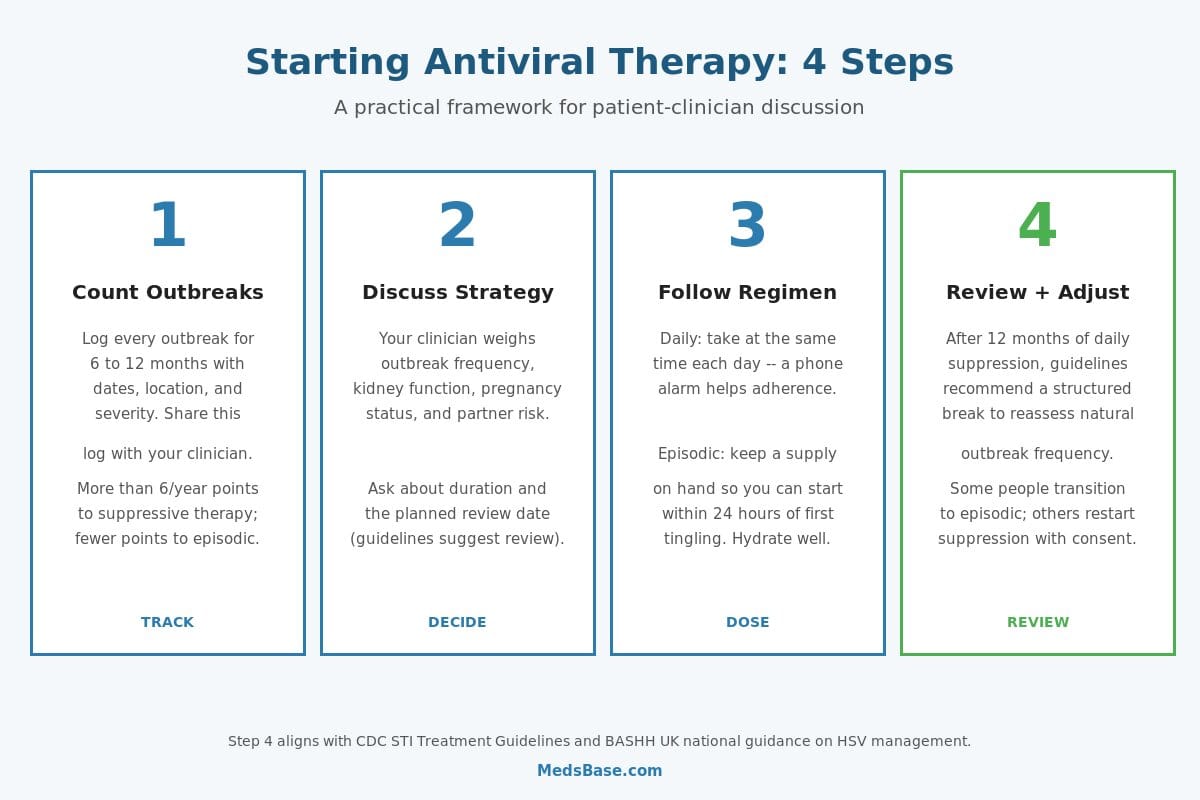
How to Start Antiviral Therapy — Practical Guidance
The decision is not really daily-or-episodic in the abstract — it is daily-or-episodic for you, based on outbreak pattern, partner status, life stage, and how much a pill a day fits your routine.
Step 1 — Track Outbreaks for 6 to 12 Months
Before committing to daily therapy, most clinicians want a baseline outbreak diary: date, location, severity, and duration of every outbreak over 6–12 months. A phone note or calendar entry is enough. This single data point guides everything downstream.
Step 2 — Discuss the Strategy with a Clinician
Your clinician will weigh outbreak frequency, kidney function, pregnancy status, HSV status of any sexual partner, and your preferences about pill-taking. If cost is a factor, generic acyclovir is typically the least expensive option; if dosing simplicity matters most, valacyclovir once daily wins.
Step 3 — Follow the Regimen Consistently
On daily therapy, take the pill at the same time each day — a phone alarm is a common and effective trick. Missed doses are forgiving over a day or two, but sustained gaps erode the protective effect. On episodic therapy, keep a spare supply at home and at work so you can start treatment within hours of the first tingling, not hours of getting home.
Step 4 — Review and Adjust at 12 Months
The CDC and BASHH both recommend reviewing suppressive therapy after about 12 months — not to stop it automatically, but to see whether the underlying outbreak pattern has changed. Some people discover the natural recurrence rate has dropped below a level worth suppressing; others confirm they still need it. Either answer is valid.
Browse our range of herpes antivirals including Valclovir (generic valacyclovir) and Centrex tablets at MedsBase.
Frequently Asked Questions
Is daily suppressive therapy safe to take for years?
Long-term follow-up studies of acyclovir have followed patients on daily therapy for 10–20 years without finding cumulative toxicity. Periodic kidney-function monitoring is reasonable, and most guidelines suggest a review at 12 months to reassess whether continued suppression is still needed — but the safety evidence for multi-year use is strong.
Can I switch between daily and episodic treatment?
Yes, and many people do. A typical pattern is daily suppression during high-stress periods, pregnancy, or a new relationship, followed by a transition to episodic treatment once outbreaks are less frequent. Any switch should be discussed with your clinician, but neither strategy prevents you from moving to the other later.
Does daily valacyclovir prevent me from passing herpes to my partner?
Daily valacyclovir reduces the risk of passing HSV-2 to a susceptible partner by about 48%, according to the Corey 2004 trial in the New England Journal of Medicine. It does not eliminate transmission risk — consistent condom use, avoiding sex during outbreaks, and open communication remain important layers of protection alongside antiviral therapy.
How quickly must I start episodic treatment for it to work?
The ideal window is within 6 hours of first symptoms — the prodromal tingling, itching, or burning that precedes visible lesions. Treatment started within 24 hours still shortens outbreaks meaningfully. Beyond 48 hours the benefit drops off sharply, because most viral replication has already occurred by then.
Which antiviral is best for cold sores versus genital herpes?
Any of the three main antivirals work for both sites, but for cold sores single-day high-dose regimens (valacyclovir 2 g twice in a day, or famciclovir 1.5 g once) are particularly convenient. For genital herpes, valacyclovir 500 mg twice daily for 3 days is the most commonly prescribed episodic course because the twice-daily schedule is easier to stick to than acyclovir’s five-times-a-day regimen.
Will herpes antivirals interact with other medications I take?
Clinically important interactions are uncommon. Caution is needed with nephrotoxic drugs (some NSAIDs taken chronically, aminoglycosides, tenofovir) because they compound renal exposure. Probenecid raises antiviral blood levels by slowing kidney clearance. Always share a full medication list with your prescriber, including over-the-counter drugs and supplements.
Do I still need antivirals if I rarely get outbreaks?
Not necessarily. If you get fewer than two outbreaks a year and they are mild, no treatment at all is a valid option. Many people in this category keep a short episodic supply on hand for the occasional flare and never take a daily pill. The strongest argument for daily therapy in this group is transmission reduction to a susceptible partner.
What happens if I stop daily suppressive therapy?
Outbreak frequency usually returns to your pre-treatment baseline over the following weeks to months. Some people find their natural pattern has improved (HSV-2 recurrence rates tend to decline slowly over years) and manage comfortably without medication. Others see the old pattern resume and restart suppression. Stopping is fully reversible and does not damage future response to the drug.
The Bottom Line
There is no single right answer to daily vs episodic herpes antiviral treatment — the right answer depends on how often you get outbreaks, whether you have a susceptible partner, and how you personally weigh a daily pill against reactive treatment.
Daily suppressive therapy is the strategy of choice when outbreaks are frequent, when you want the best available reduction in transmission risk, or when immune suppression raises the stakes of a severe outbreak. The evidence is mature: roughly 70–80% fewer outbreaks, a 48% lower transmission rate to a susceptible partner, and a safety profile that holds up across decades of use.
Episodic therapy is the rational choice when outbreaks are infrequent, prodromal symptoms are reliable, and the priority is shortening the occasional outbreak rather than preventing all of them. It avoids the daily-pill routine and the cost of continuous dosing, and it performs very well on its own terms — 1–2 days off each outbreak with no preventive obligation between flares.
For most people, the best approach is a conversation with a clinician that starts with an outbreak diary and ends with a plan reviewed at 12 months. Whatever strategy you choose, the medicines themselves have held up to 40 years of scrutiny with an enviable safety record — the decision is about fit, not efficacy.
Ready to discuss a plan with your clinician? Browse our sexual health category for generic valacyclovir, Centrex, and other HSV antivirals. For more background, see our guides to how aciclovir works in genital herpes and genital herpes symptoms.
![]()
Reviewed by the MedsBase Editorial Team
Last updated: 18 April 2026
Selected references: Reitano M et al. J Infect Dis 1998;178:603–10. Mertz GJ et al. Arch Intern Med 1997;157:343–9. Diaz-Mitoma F et al. JAMA 1998;280:887–92. Corey L et al. N Engl J Med 2004;350:11–20. WHO HSV Fact Sheet 2024. CDC STI Treatment Guidelines 2021. BASHH UK National Guideline for the Management of Anogenital Herpes 2024.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.