







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
By age 50, about half of all men show some degree of male pattern hair loss. Two prescription drugs have dominated the medical side of that fight for nearly three decades: finasteride and dutasteride. Both work on the same pathway. Both are daily oral tablets. Both are widely available generically. And on paper they look almost identical — until you look closely.
If you’re weighing finasteride vs dutasteride — whether starting treatment for the first time, considering a switch because finasteride has plateaued, or trying to understand the real-world trade-offs — this guide covers exactly what separates them. You’ll see how each drug works at the enzymatic level, what the head-to-head and network meta-analysis data actually show, how the side-effect profiles compare, the half-life gap most comparisons skip, and who tends to benefit more from each.
- Finasteride blocks Type II 5α-reductase; dutasteride blocks both Type I and Type II — producing more complete DHT suppression (~92% vs ~73% of serum DHT).
- Two independent network meta-analyses (2022 and 2025) rank dutasteride 0.5 mg ahead of finasteride 1 mg on hair count — but the efficacy edge is modest and the evidence certainty is rated low.
- Only finasteride is FDA-approved for androgenetic alopecia (AGA). Dutasteride is approved for hair loss in South Korea and Japan; used off-label in the US, UK, and EU.
- Side-effect profiles are broadly similar — sexual side effects in low single-digit percentages, typically reversible on discontinuation.
- Dutasteride’s half-life is ~5 weeks versus finasteride’s 5–6 hours; this matters for washout periods, blood donation, fertility planning, and post-treatment recovery.
What Are Finasteride and Dutasteride?
Finasteride and dutasteride are both oral prescription medications in a drug class called 5α-reductase inhibitors (5-ARIs). They block the enzyme that converts testosterone into dihydrotestosterone (DHT) — the hormone primarily responsible for male pattern hair loss and benign prostate enlargement.
Finasteride was FDA-approved in 1992 (as Proscar 5 mg) for benign prostatic hyperplasia (BPH) and in 1997 (as Propecia 1 mg) for male pattern hair loss. It was the first 5α-reductase inhibitor in clinical use and remains the only one with FDA approval for androgenetic alopecia in men.
Dutasteride was FDA-approved in 2001 (as Avodart 0.5 mg) for BPH. It is a dual inhibitor, blocking both Type I and Type II 5α-reductase isoenzymes. Although extensive clinical data support its efficacy for hair loss, the FDA has never approved it for that indication — but the South Korean regulator approved it for AGA in 2009, and Japan followed in 2015 (as Avolve/Zagallo). US and European prescribers use it off-label, most often after finasteride has plateaued or caused intolerable side effects. That off-label status is a genuine trade-off, not a technicality — we cover it honestly below rather than treating dutasteride as a hidden upgrade.
The single structural difference — inhibiting one isoenzyme versus both — is responsible for most of the clinically meaningful differences between them.
How Do Finasteride and Dutasteride Work?
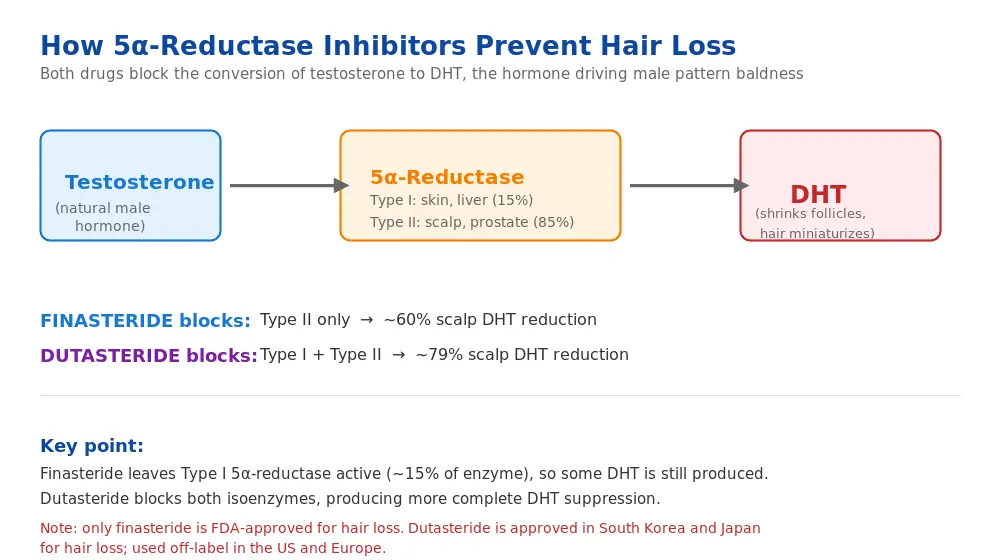
Male pattern baldness is driven by a hormone called dihydrotestosterone (DHT). DHT is about three times more potent than testosterone at binding to androgen receptors. In genetically susceptible men, DHT binds to receptors inside scalp hair follicles and triggers progressive miniaturisation — the follicle shrinks, the hair it produces becomes thinner and shorter, and eventually the follicle stops producing terminal hair entirely.
Testosterone is converted to DHT by an enzyme called 5α-reductase, which exists in two major isoforms:
- Type I — predominantly in skin (including sebaceous glands), liver, and certain parts of the brain. Accounts for about 15% of total DHT production in the body.
- Type II — predominantly in hair follicles, the prostate, and male reproductive tissues. Accounts for the majority of DHT production in androgen-sensitive tissues. About 85% of total DHT production.
Finasteride selectively inhibits Type II 5α-reductase. At the standard 1 mg daily dose, it reduces serum DHT by roughly 70–73% and scalp DHT by about 60%. Crucially, it leaves Type I activity intact, meaning some DHT continues to be produced from the skin and liver isoenzyme.
Dutasteride is a dual inhibitor — it blocks both Type I and Type II 5α-reductase. At 0.5 mg daily, it reduces serum DHT by over 90% (roughly 92% in pooled data) and scalp DHT by approximately 79%. Because it shuts down nearly all 5α-reductase activity across both isoforms, the DHT suppression is more complete.
In practice, that extra suppression translates into measurably better hair-count outcomes — but also into a longer pharmacological shadow, because dutasteride’s half-life is dramatically longer than finasteride’s, a difference we return to in the safety section.
Key Uses and Who Each Drug Is For
Both drugs are used for two overlapping conditions: male pattern hair loss and benign prostate enlargement. Their real-world fit varies.
Androgenetic Alopecia (Male Pattern Hair Loss)
This is where most patients encounter these drugs. Both produce meaningful slowing of hair loss, stabilisation of existing follicles, and — for a majority of users — visible regrowth in the crown and mid-scalp areas. The frontal hairline typically responds less.
Finasteride 1 mg daily is the standard first-line pharmacological treatment. If you and a prescriber settle on it, the generic version — sold as generic finasteride 1 mg — is the identical molecule at the same dose as the brand; our brand vs generic finasteride breakdown answers the “is generic really as good?” question in detail. Dutasteride 0.5 mg daily is typically used when finasteride has plateaued, produced insufficient regrowth, or when a patient specifically wants maximum DHT suppression.
Benign Prostatic Hyperplasia (BPH)
Both drugs shrink the prostate gland and relieve urinary symptoms in men with BPH. At higher doses (finasteride 5 mg as Proscar, dutasteride 0.5 mg as Avodart), they reduce prostate volume by 18–28% over 6–12 months and improve urinary flow. Dutasteride has slightly stronger BPH data in men with very large prostates.
Hair Transplant Support
Both drugs are commonly prescribed before and after hair transplant surgery to preserve non-transplanted native hair and prevent progression of the underlying miniaturisation process. Without ongoing pharmacological support, transplanted hair stays but surrounding native hair continues to thin.
Other Emerging or Off-Label Uses
- Female pattern hair loss: used off-label in postmenopausal women; contraindicated in women of reproductive potential due to severe teratogenic risk
- Gender-affirming care: occasionally used in transgender women as an adjunct to estrogen therapy
- Hirsutism: off-label use in women with hormonally-driven excess body hair
- Prostate cancer risk reduction: both drugs reduce the incidence of low-grade prostate cancer in men taking them long-term, though this remains controversial due to a small signal of high-grade tumours in trials
Safety Profile, Side Effects, and the Half-Life Gap
Finasteride and dutasteride can cause serious birth defects in a developing male fetus. Women who are pregnant, may become pregnant, or are breastfeeding must not take these medicines — and must not handle crushed or broken finasteride tablets or leaking dutasteride capsules, because the drug can be absorbed through the skin. Per MedlinePlus finasteride information and MedlinePlus dutasteride information, both should be stored securely away from anyone who could be pregnant. This is the one area of the whole comparison where the guidance is firm, not qualified: there is no safe handling exception.
Half-Life and Washout — the Difference Most Comparisons Skip
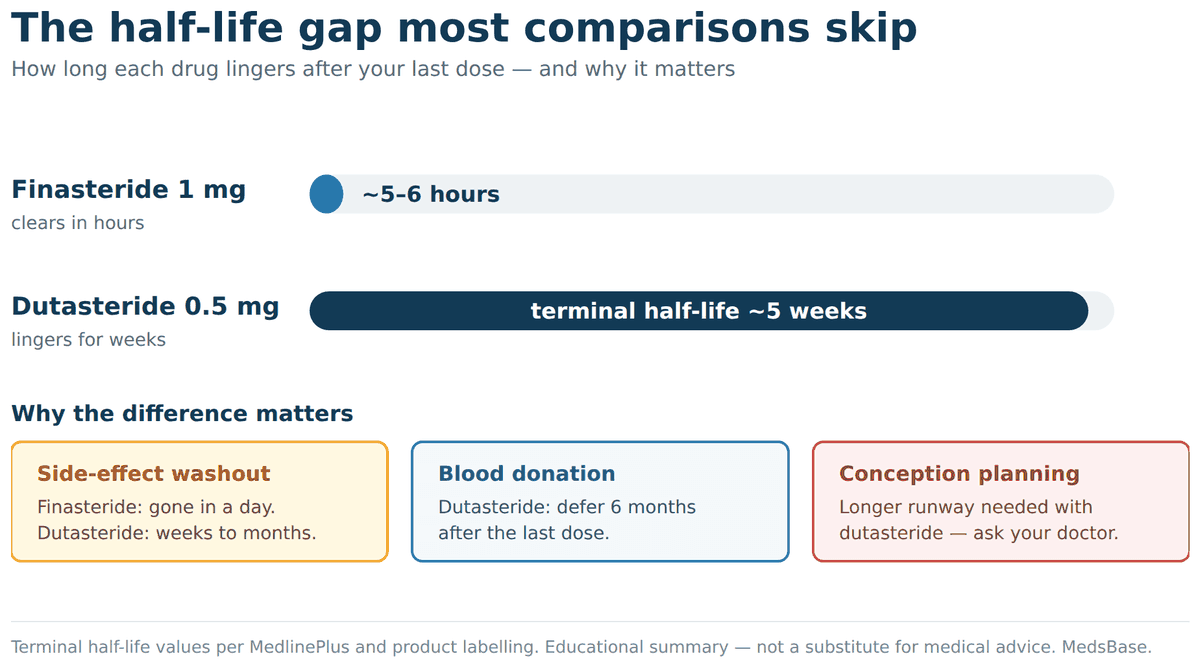
Finasteride has a short half-life of roughly 5–6 hours. Dutasteride’s terminal half-life is about five weeks. That single fact ripples through several real-world decisions:
- Side-effect washout. If finasteride causes an unwanted effect, stopping it clears the drug within about a day. If dutasteride does, the molecule can linger for weeks to months — so any adverse effect fades far more slowly.
- Blood donation. Because dutasteride persists, guidance says don’t donate blood while taking it or for six months after stopping (to protect a potentially pregnant recipient). Finasteride carries a shorter deferral, commonly cited as around one month after the last dose.
- Conception planning. Men trying to conceive should discuss timing with their doctor. The teratogenic risk is to a developing male fetus via a partner’s exposure — not a reason for panic, but a reason for a conversation and, with dutasteride, a longer runway.
Side-Effect Frequency (Controlled Trial Data)
| Side effect | Finasteride 1 mg | Dutasteride 0.5 mg | Severity (most cases) |
|---|---|---|---|
| Decreased libido | 1.8% | 3.0% | Mild, usually reversible |
| Erectile dysfunction | 1.3% | 2.5% | Mild–moderate, usually reversible |
| Ejaculation disorder | 1.2% | 1.4% | Mild |
| Gynaecomastia / breast tenderness | 0.4% | 0.8% | Mild, reversible on stopping |
| Depression / mood changes | 0.3% | 0.3% | Variable, monitored |
| Testicular pain | 0.2% | 0.3% | Mild, uncommon |
| Reduced ejaculate volume | 0.8% | 1.1% | Mild, reversible |
| Lowered PSA reading | Expected (~50%) | Expected (~50%) | Lab effect — tell your doctor |
| Persistent post-drug symptoms | Rare, debated | Rare, debated | Controversial (see below) |
Data pooled from Propecia labelling (Merck), Avodart labelling (GSK), and head-to-head trial data. In most studies, the absolute difference in side-effect frequency between the two drugs is small and not always statistically significant. There is also a genuine nocebo effect in this area: men told to expect sexual side effects report them more often, which makes the true attributable rate hard to pin down — honest uncertainty is the correct stance.
The Post-Finasteride Syndrome (PFS) Debate
A subset of users — the reported rate varies from around 1.4% in some post-marketing analyses to under 0.1% in manufacturer trials — describe persistent sexual, cognitive, or emotional symptoms that do not resolve after stopping the drug. This has been labelled “post-finasteride syndrome” (PFS) or “post-5ARI syndrome.”
The clinical and scientific community remains divided. Some researchers argue for a genuine neuroendocrine mechanism (possibly via altered neurosteroid synthesis); others point to confounding factors (baseline rates, nocebo effect, underlying depression). Regulatory agencies in France, the UK, and several other countries have updated labelling to mention persistent symptoms; US FDA labelling has been updated more cautiously. If this is your main concern, our balanced look at the post-finasteride syndrome debate covers what the evidence does and doesn’t show.
Practical guidance: any patient considering either drug should be briefed on this possibility, particularly if they have a history of depression or anxiety. Stopping at the first sign of mood or sexual symptoms — rather than pushing through — appears to reduce the risk of persistent effects.
Contraindications (Both Drugs)
- Pregnancy / women of reproductive potential: severe teratogenic risk (male fetal genital development). Women should not even handle crushed or broken tablets or capsule contents.
- Active liver disease: both drugs are extensively metabolised by the liver.
- Personal history of severe depression: use with caution; close monitoring recommended.
- Known hypersensitivity to finasteride, dutasteride, or related 5-ARIs.
What Does the Research Say?

The evidence base on both drugs is now extensive, and the most recent data both settles and unsettles the debate. Two independent network meta-analyses — studies that statistically pool many trials to rank treatments — point the same direction.
A 2025 network meta-analysis of 33 studies (published in the Journal of Cosmetic Dermatology) ranked oral dutasteride 0.5 mg as the most effective monotherapy for male pattern hair loss, ahead of finasteride 1 mg, attributing the edge to its deeper 92%-versus-73% serum DHT suppression. An earlier 2022 network meta-analysis of 23 studies (Gupta et al., JAMA Dermatology) found dutasteride 0.5 mg beat finasteride 1 mg on 24-week total hair count by about +7.1 hairs/cm² (95% CI 5.1–9.3) — but explicitly rated the certainty of that comparison as low.
That “low certainty” flag is the number that should temper expectations. A statistically real edge built on limited, heterogeneous data is a reason to consider dutasteride, not a mandate to demand it.
Dosing frequency is an active question too. A 2025 investigator-blinded pilot RCT in JAAD International tested twice- and thrice-weekly dutasteride against daily finasteride in 60 men over 24 weeks. Thrice-weekly dutasteride produced a numerically higher terminal hair count than daily finasteride (17.4 vs 12.8 hairs/cm²), though the difference was not statistically significant (P = 0.23), and sexual side effects were similar across all three groups. It’s a small pilot — a promising signal that dutasteride’s long half-life might allow less-than-daily dosing, not proof.
| Study | Year | Key finding | Source |
|---|---|---|---|
| Kaufman et al. | 1998 | 86% of finasteride 1 mg users had no further hair loss at 5 years | JAAD (5-year AGA trial) |
| Olsen et al. | 2006 | Dutasteride 0.5 mg reduced scalp DHT more than finasteride 5 mg | JAAD (dose-ranging) |
| Harcha et al. | 2014 | Head-to-head (n=917, 24 wks): dutasteride +94.6 vs finasteride +78.5 hairs/cm² | JAAD (head-to-head RCT) |
| Gupta et al. (23 studies) | 2022 | Dutasteride 0.5 mg > finasteride 1 mg by +7.1 hairs/cm² at 24 wks; evidence quality low | JAMA Dermatology |
| Network meta-analysis (33 studies) | 2025 | Dutasteride 0.5 mg ranked most effective monotherapy; ~92% vs ~73% DHT suppression | J Cosmet Dermatol |
| Investigator-blinded pilot RCT (n=60) | 2025 | Thrice-weekly dutasteride numerically ≥ daily finasteride (not significant); similar sexual side effects | JAAD International |
Research suggests — consistently across multiple studies — that dutasteride’s efficacy advantage over finasteride is real but moderate. It is not a paradigm shift, but a reliable, modest edge in most head-to-head and pooled comparisons.
The biggest practical caveat: long-term safety data on dutasteride specifically for AGA (beyond about two years) are thinner than finasteride’s, which now has 25+ years of post-marketing use. That is one reason regulatory agencies have been slower to approve dutasteride for hair loss.
Finasteride vs Dutasteride — Direct Comparison Table
| Criterion | Finasteride | Dutasteride |
|---|---|---|
| Mechanism | Type II 5α-reductase inhibitor | Dual Type I + II 5α-reductase inhibitor |
| Brand names | Propecia, Proscar, Finpecia, Finrest | Avodart, Dutas, Dutas-T, Avolve |
| Hair loss dose | 1 mg once daily | 0.5 mg once daily |
| BPH dose | 5 mg once daily | 0.5 mg once daily |
| FDA approval for hair loss | Yes (1997) | No (BPH-approved; used off-label) |
| Half-life | 5–6 hours | ~5 weeks |
| Serum DHT reduction | ~70–73% | ~92% |
| Scalp DHT reduction at 12 months | ~60% | ~79% |
| Hair count increase (6 mo, Harcha) | +78.5 hairs/cm² | +94.6 hairs/cm² |
| Sexual side-effect rate | ~2–3% | ~3–4% |
| Long-term safety data | 25+ years | ~20+ years (less AGA-specific) |
| Blood donation deferral | ~1 month after last dose | 6 months after last dose |
| Typical monthly cost (generic) | $5–25 USD | $10–35 USD |
How to Use Each Drug Safely
Both drugs follow simple daily dosing schedules. Unlike titrated medications, there is no ramp-up — you start on the therapeutic dose from day one.
Finasteride (for Hair Loss)
- Dose: 1 mg once daily, with or without food
- Timing: at roughly the same time each day
- Expected onset: reduced shedding within 2–3 months; visible regrowth from month 4 onward; full effect assessed at 12 months
- Duration: indefinite for continued benefit; stopping reverses gains over 6–12 months
Dutasteride (for Hair Loss, Off-Label in US/EU)
- Dose: 0.5 mg once daily (swallow whole, don’t crush or chew)
- Timing: with or without food, same time daily
- Expected onset: similar to finasteride but ramp may be slightly faster due to greater DHT suppression; some protocols use 0.5 mg two-to-three times weekly for reduced exposure
- Duration: indefinite for continued benefit; due to long half-life, effects linger 5–6 months after stopping
Practical Guidance (Both Drugs)
- Take consistently — missing occasional doses is fine, but extended interruptions cause hair regrowth to reverse
- Most users combine 5-ARI therapy with minoxidil 5% topical; because the two work on different mechanisms, pairing them is one of the most evidence-supported strategies in male hair loss. A ready-made finasteride-plus-minoxidil stack bundles both if a clinician agrees that’s your route.
- Expect an initial “shedding phase” in the first 2–8 weeks as miniaturised follicles cycle out to be replaced by healthier ones — this is a sign the drug is working, not a sign to stop
- Give it real time: 5-ARIs need 6–12 months before you can fairly judge them, so track standardised monthly photos rather than going by feel
- Tell any doctor ordering a PSA test that you take a 5-ARI — both drugs roughly halve PSA and the reading must be interpreted accordingly
- Fertility: both drugs reduce ejaculate volume slightly and may transiently reduce sperm count; men actively trying to conceive may wish to pause (especially dutasteride, whose long half-life means 6+ months of washout)
- Women of reproductive age must not handle broken or crushed tablets or capsule contents — severe teratogenic risk
One honest catalogue note, so you don’t order the wrong thing: the dutasteride-containing product on our shelves, Dutas-T, is a BPH combination of dutasteride 0.5 mg plus tamsulosin 0.4 mg — formulated for prostate symptoms, not hair loss. Any decision to use dutasteride for the scalp is an off-label call to make with your prescriber.
Cost Comparison
Both drugs are available as inexpensive generics globally. Brand-name pricing remains higher in some markets but is rarely the best option.
- Finasteride 1 mg (generic): roughly $5–25/month for a 30-day supply in most markets, produced by WHO-GMP-certified manufacturers such as Cipla (Finpecia) and Dr. Reddy’s (Finrest). Brand Propecia runs $50–80/month in the US without insurance.
- Dutasteride 0.5 mg (generic): roughly $10–35/month for a 30-day supply, produced by WHO-GMP-certified manufacturers such as Dr. Reddy’s (Dutas) and Cipla (Duprost). Brand Avodart runs $100–150/month in the US without insurance.
The practical cost difference between the two is small. For most patients, the choice comes down to efficacy and tolerability, not price.
Can You Switch Between Finasteride and Dutasteride?
Yes, and this is a common clinical scenario. Most patients start on finasteride (because it’s FDA-approved, cheaper, and has longer safety data), then switch to dutasteride if they plateau or want more aggressive DHT suppression. Weighing the dutasteride brands specifically? Our Avodart vs generic dutasteride comparison covers that choice.
Switching from finasteride to dutasteride: no washout is required. You can stop finasteride today and start dutasteride tomorrow. Many protocols do exactly this when a patient plateaus on finasteride after 12–18 months.
Switching from dutasteride to finasteride: because dutasteride has a half-life of about 5 weeks, it remains detectable in serum for up to 6 months after the last dose. Starting finasteride during that washout is safe (no drug interaction) — it just means DHT suppression will remain high for several months regardless.
Stopping either drug entirely: DHT levels rebound within 1–2 weeks for finasteride and over 4–6 months for dutasteride. Hair gains typically erode over the following 6–12 months as the underlying miniaturisation process resumes.
Common reasons to switch:
- Plateau on finasteride after 12–18 months of initial response
- Intolerable side effects on one drug that may not replicate on the other
- Cost differences in local markets
- Supply issues
Reasons some patients stay on finasteride despite dutasteride’s higher efficacy:
- Longer safety track record (25+ years of post-marketing data)
- Shorter half-life — side effects clear faster if they occur
- FDA approval for AGA (prescriber and patient confidence)
- Slightly lower sexual side-effect rate in most pooled data
Frequently Asked Questions
Is dutasteride stronger than finasteride for hair loss?
Yes, in terms of pharmacological potency and clinical efficacy. Dutasteride blocks both isoforms of 5α-reductase and suppresses serum DHT by about 92% versus finasteride’s ~70–73%. Two network meta-analyses rank dutasteride 0.5 mg ahead of finasteride 1 mg for hair count. That said, the edge is modest, the certainty is rated low, and “stronger” also means a slightly higher side-effect rate and a much longer half-life — so the choice is not automatic and belongs with your clinician.
Is dutasteride FDA-approved for hair loss?
No. In the United States, dutasteride is FDA-approved for benign prostatic hyperplasia (enlarged prostate), and using it for hair loss is off-label. Finasteride 1 mg is the one FDA-approved for male androgenetic alopecia. Notably, dutasteride is approved specifically for hair loss in South Korea and Japan — approval standards differ by country, which is why “not approved for hair” is a US-and-Europe statement, not a global one.
Can I take finasteride and dutasteride together?
No. Taking both simultaneously offers no additional benefit because dutasteride already blocks everything finasteride blocks, plus the Type I enzyme finasteride doesn’t touch. Combining them just increases side-effect risk with no efficacy gain. If finasteride isn’t working well enough, the standard approach is to switch to dutasteride, not add it.
How long does dutasteride stay in your system?
A long time. Dutasteride’s terminal half-life is roughly five weeks, so it can remain measurable in your blood for weeks to months after your last dose. That’s why blood-donation guidance says to wait six months after stopping, and why any side effect fades more slowly than it would with short-acting finasteride (5–6 hours).
How long does it take to see results?
Expect reduced shedding within 2–3 months, visible regrowth in the crown and mid-scalp from month 4, and full effect assessed at 12 months for both drugs. Dutasteride may produce slightly faster initial improvement in some users due to its higher DHT suppression, but the 12-month endpoint is the standard clinical assessment for both.
Are the side effects reversible?
For most users, yes — sexual side effects and breast tenderness resolve within weeks of stopping finasteride, though dutasteride’s longer half-life means effects can take 2–6 months to fully wash out. A small minority of users report persistent symptoms (“post-finasteride syndrome” / PFS), which remains a debated phenomenon. If any mood, libido, or erectile changes appear, stopping early rather than pushing through is the safer approach.
Can women take finasteride or dutasteride?
Both drugs are contraindicated in women of reproductive potential due to severe risk of genital malformation in male fetuses — women should not even handle crushed or broken tablets or capsule contents. In postmenopausal women with female pattern hair loss, finasteride (and rarely dutasteride) is sometimes used off-label, but only under specialist supervision and with clear counselling about limited evidence.
Does either drug affect PSA levels for prostate cancer screening?
Yes — both drugs suppress PSA by roughly 50% within 3–6 months of starting. Any prostate cancer screening on either drug must use doubled PSA values or compare to a baseline taken before starting. Tell your GP or urologist you’re taking a 5-ARI before any PSA test.
Do I need a prescription for finasteride or dutasteride?
These are clinician-guided medicines, and MedsBase does not require you to upload a prescription to order — no prescription needed to browse or buy. That convenience does not replace medical judgement: both drugs affect fertility, mood risk, and PSA testing, so the decision to start, switch, or stop is best made with a doctor or pharmacist rather than self-directed from a comparison table.
The Bottom Line
Finasteride and dutasteride are the two most effective prescription drugs for male pattern hair loss, and neither is universally “better.” The honest verdict:
- For first-time treatment, finasteride remains the standard starting point — FDA-approved, 25+ years of safety data, inexpensive, shorter half-life, and effective in the majority of users.
- For maximum efficacy or after finasteride plateaus, dutasteride produces a modest but reliable hair-count advantage with broadly similar tolerability, though off-label for AGA in most jurisdictions and built on lower-certainty evidence.
- For short pharmacological exposure (e.g. men considering near-term fertility, or those wanting to minimise wash-out if side effects occur), finasteride’s 5–6 hour half-life is a meaningful advantage over dutasteride’s five weeks.
- For cost, both are inexpensive generically; the difference is usually not a deciding factor.
Most users get excellent long-term results on finasteride monotherapy (combined with topical minoxidil 5%). Dutasteride is best reserved for the subset who want more aggressive suppression, have plateaued on finasteride, or have access to a prescriber comfortable using it off-label. Whichever way you lean, the one action worth taking today is a conversation with a clinician — and if you have a PSA test, mention either drug, because it changes how the result is read.
Browse the full hair loss treatment for men range for finasteride, dutasteride, and combination options, or read our brand vs generic finasteride guide if you’re still deciding whether the generic is as good as the brand.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.