







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

Six months into semaglutide. Down about 40 pounds. You reach for the trainers you’ve worn all year — and your heel slides up and down with every step, like the shoe suddenly belongs to someone bigger. The skin across the top of your foot looks a little softer than it used to. Nothing hurts, exactly. But something is clearly different, and a video you scrolled past last night gave it a name: Ozempic feet.
If that scenario feels close to home, you’re in the right place. Ozempic feet is the nickname for the foot changes some people notice during rapid GLP-1 weight loss — looser shoes, thinner cushioning underfoot, and skin that hangs a touch more than it did. It sounds alarming. Most of the time, it isn’t. But there’s one situation where new foot symptoms are a genuine warning sign, and we’ll get to exactly how to tell the difference.
By the end of this guide you’ll understand what’s really happening inside your feet, who tends to notice it most, when a change is cosmetic versus when it needs a clinician, and five practical fixes that actually help. One of those fixes surprises almost everyone — it has nothing to do with your feet at all.
Key Takeaways
- “Ozempic feet” is not a drug toxicity — it tracks the amount and speed of your weight loss, and one comparison table later makes that unmistakable.
- Your feet hold shock-absorbing fat pads; lose enough total-body fat and those can thin too — but there’s a reason older skin sags more than younger skin.
- The evidence here is observational and dermatologic commentary, not hard clinical proof — and we say so plainly instead of overselling it.
- There’s one red flag that is never just “Ozempic feet” — miss it and you could miss something serious.
- Four of the five fixes are things you can start this week; the fifth is knowing when to book a podiatrist.
On this page
What Is “Ozempic Feet”?
Let’s clear up the name first, because the name is doing a lot of misleading work. There is no ingredient in semaglutide that targets your feet. Ozempic and Wegovy (both brand names for semaglutide) are GLP-1 receptor agonists that reduce appetite and slow stomach emptying, which lowers how much you eat. The result is body-wide fat loss. Your feet are simply part of your body — so when fat leaves, some of it leaves your feet too.
The phrase caught fire the same way “Ozempic face” did: people described a visible change, social media gave it a catchy label, and suddenly a normal consequence of weight loss looked like a mysterious new syndrome. It isn’t mysterious. It’s biology you can actually understand in about three minutes.
Here’s the honest framing you won’t get from a viral clip. Ozempic feet is a story about the amount and speed of weight loss, not about the drug attacking your feet. Lose the same amount of weight the same fast way through any method, and you’d expect the same feet. Keep that idea in your back pocket — it’s the thread that ties this whole article together, and there’s a comparison table coming that proves it.
How Does Ozempic Feet Happen? (The Honest Mechanism)
Think of the sole of your foot like the sole of a running shoe. Under your heel and under the ball of your foot sit specialised fat pads — the heel (calcaneal) pad and the plantar fat pad. They’re not spare padding your body forgot about. They’re engineered shock absorbers, packed into tough little chambers that spread the load every time your heel strikes the ground. Without them, walking would feel like standing on bare bone.

Now, two things happen when you lose a lot of weight quickly.
First, fat pads can shrink. Your body doesn’t let you choose where fat comes off. When you drop a large percentage of total body fat — the kind of loss GLP-1 medications can drive — some of that comes from the cushioning in your feet. Thinner pads mean less padding between bone and pavement, which is why some people feel the ground more than they used to.
Second, skin doesn’t snap back as fast as fat disappears. Your skin has elastic scaffolding — collagen and elastin — that lets it retract as you shrink. But that scaffolding retracts on its own timeline. When fat volume drops faster than skin can catch up, you get loose skin. On the feet, that shows up as softer, slightly saggy skin over the top of the foot and around the ankle. Dermatology commentary on GLP-1 agonists describes exactly this lag between rapid volume loss and skin retraction (dermatology commentary on GLP-1 agonists and skin health, open-access review).
How much weight are we talking about? In the STEP 1 trial published in the New England Journal of Medicine (PubMed record), adults on once-weekly semaglutide lost on average close to 15% of their body weight over 68 weeks. For someone starting at 250 pounds, that’s around 37 pounds — a big enough shift that visible changes anywhere on the body, feet included, are entirely predictable.
Research Spotlight
The heel-pad connection isn’t hand-waving. A case-control study found that people with thinner subcalcaneal (heel) fat pads had more plantar heel pain than those with thicker pads (thinner heel fat pads are linked to plantar heel pain). That’s the plausible bridge between losing pad thickness and feeling new discomfort underfoot. It does not prove semaglutide thins heel pads directly — no trial has measured that — which is exactly the kind of honesty this topic needs.
Here’s where we have to be straight with you, because most coverage isn’t. The evidence base for “Ozempic feet” is observational and dermatologic — anecdote collection plus general weight-loss and fat-pad science — not dedicated clinical trials on GLP-1 users’ feet. We know fat pads thin with fat loss. We know skin lags. We know GLP-1 drugs cause significant loss. Connecting those dots is reasonable, but it’s inference, not a proven cause-and-effect chain measured in a study. Anyone who tells you it’s settled science is overselling it.
What People Actually Notice — And Who Notices Most
The changes people report cluster into a handful of experiences. If you’ve felt one, you’ve probably felt two:
- Shoes fit looser — especially heel slippage, the classic first clue.
- Thinner cushioning underfoot — you feel hard floors and pavement more.
- A half-size shoe drop — some people genuinely go down a size as swelling and fat both reduce.
- Sagging or crepey skin on the top of the foot and around the ankle.
- Tendons and veins look more visible as the fat layer over them thins.
- New pressure points or blisters because old shoes now rub in new places.

Not everyone gets all of these, and plenty of GLP-1 users notice none. So who tends to notice the most? Three factors stack the odds:
- Older skin. Collagen and elastin decline with age, so skin retracts more slowly. A 30-year-old and a 60-year-old can lose the same weight and end up with very different amounts of loose skin.
- Faster loss. The quicker the drop, the less time skin and supporting tissue have to adapt. Speed matters as much as the total.
- Higher starting weight. A larger total amount of fat to lose means a bigger visible change when it goes.
If you’re older, losing fast, and started from a higher weight, you’re in the group most likely to see Ozempic feet — and none of that means anything has gone wrong. It means your body is doing the thing you asked it to do, just faster than your skin’s repair crew can keep pace.
One pharmacist observation worth sharing: people are often blindsided by foot changes precisely because nobody warned them. They brace for nausea and appetite changes, not for their trainers to feel roomy. Knowing it can happen turns a scary surprise into a manageable, expected footnote.
When Foot Changes Matter Medically (Read This Part)
Most Ozempic feet changes are cosmetic or mildly uncomfortable. But “most” isn’t “all,” and this is the section to slow down on.
Foot changes cross from cosmetic into medical when they start affecting how you move and what your skin can tolerate:
- New heel or arch pain that shows up with thinner cushioning — the fat-pad-thinning link is real, and pain that limits your walking deserves attention.
- Gait changes — if your feet hurt, you unconsciously alter how you walk, which can push strain into your knees, hips, and back.
- Ill-fitting shoes causing blisters or pressure sores — loose shoes rub; rubbing breaks skin; broken skin can get infected.
Any of those is a good reason to reassess your footwear and, if it persists, see a podiatrist. That’s ordinary, fixable stuff.
Then there is the one situation that is never just “Ozempic feet.”
Diabetes Foot Red Flag — Do Not Ignore This
Many people taking semaglutide have type 2 diabetes. Diabetic nerve damage (neuropathy) and foot ulcers are NOT “Ozempic feet” — they are separate, serious conditions, and confusing the two can be dangerous.
If you have diabetes (or prediabetes) and you notice any of the following, treat it as urgent and contact a clinician promptly — do not write it off as weight-loss cosmetics:
- Numbness, tingling, burning, or loss of sensation in the feet
- A sore, blister, or cut that isn’t healing — or that you didn’t feel happen
- Redness, warmth, swelling, or drainage (possible infection)
- A change in foot shape, or new deformity
With diabetes, a small foot wound can escalate quickly because high blood sugar impairs healing and dulls the pain signals that would normally warn you. This is why anyone with diabetes and new foot symptoms needs prompt professional care — see the NIH/NIDDK guidance that anyone with diabetes and new foot symptoms needs prompt care. Loose skin is a nuisance. A missed diabetic foot ulcer is not. When in doubt, get the foot looked at.
That red-flag box is the single most important thing in this article. Cosmetic sagging can wait for your next appointment. Numbness and non-healing sores cannot.
What Does the Research Really Say?
Let’s put the evidence on the table honestly, including its limits.
| Evidence area | What it shows | Strength | Source |
|---|---|---|---|
| Semaglutide weight-loss magnitude | ~15% average body-weight loss over 68 weeks (STEP 1) | Strong — large RCT | NEJM / PubMed |
| Heel fat pad thinning & heel pain | Thinner subcalcaneal pads associated with plantar heel pain | Moderate — case-control | PubMed 30700074 |
| Rapid loss & skin laxity | GLP-1 volume loss can outpace skin retraction | Observational / dermatologic commentary | PMC review |
| GLP-1 causes foot-specific pad loss | Directly measured in a trial | Not established | No dedicated trial — general phrasing |
What this means for you: the mechanism is well-grounded in general physiology (big fat loss thins fat pads; fast loss outpaces skin), and it’s consistent with what people report. But no study has yet strapped GLP-1 users into a scanner and measured their foot pads before and after. So the correct posture is plausible and expected, not clinically proven. That distinction should make you trust this page more, not less — because it’s the truth, and it’s what a good clinician would tell you.
Ozempic Feet vs Foot Changes From Other Weight-Loss Methods
Here’s the part that dismantles the scary framing. If Ozempic feet were a drug side effect, you’d only see it in people on GLP-1 medications. You don’t. You see foot and skin changes across every method of large, fast weight loss — because the changes follow the loss, not the method.
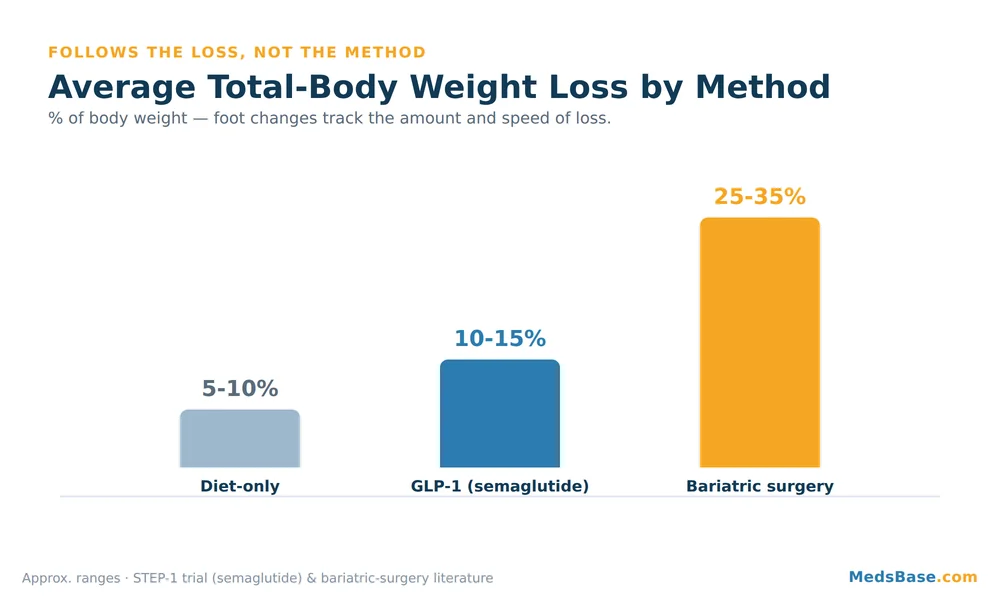
| Factor | GLP-1 (semaglutide) | Bariatric surgery | Diet-only |
|---|---|---|---|
| Typical total loss | ~10–15%+ of body weight | ~25–35% of body weight | ~5–10% (often less) |
| Typical speed | Moderate–fast (months) | Fast (12–18 months) | Slower, more gradual |
| Fat-pad thinning risk | Moderate | Highest | Lowest |
| Skin-laxity risk | Moderate | Highest | Lowest |
| Adapts with muscle/skin over time | Often, partly | Often needs longer / sometimes surgery | Usually easiest |
Which situation fits you? If you’re on a GLP-1 and losing at a steady, titrated pace, you’re in the middle of that spectrum — real changes are possible, but they’re usually milder than after bariatric surgery, and they often soften as your body composition and skin catch up. Someone losing a third of their body weight after surgery will typically see more dramatic foot and skin changes; someone trimming 8% through diet alone will usually see the least. Same phenomenon, dialled up or down by how much and how fast — not by the label on the method.
That’s the whole point, and it’s genuinely reassuring: your medication isn’t singling out your feet. Your weight loss is just doing what large weight loss does.
5 Proven Fixes for Ozempic Feet
Now the practical part — what you can actually do. Four of these you can start this week. Remember the fix that “has nothing to do with your feet”? It’s number three.

1. Pace the loss — don’t outrun your own skin.
The slower and steadier the loss, the more time your skin and tissues have to adapt, and the less dramatic the changes tend to be. That’s one reason semaglutide is meant to be titrated up gradually rather than jumped to a high dose — see the semaglutide titration schedule, which steps the dose up over roughly four months. If your loss feels alarmingly fast, that’s a conversation to have with your prescriber, not a reason to self-adjust. Curious why your rate might naturally cool off later? Here’s why weight loss stalls around month 4.
2. Fix your footwear before you fix anything else.
Thinner pads plus looser shoes is a recipe for heel slippage and blisters. Cushioned, supportive shoes and a good insole can replace some of the padding you’ve lost and stop the rubbing. Re-measure your feet — if you’ve dropped a half-size, your old shoes are now the wrong size, and heel grips or thicker socks are a cheap first fix.
3. Lift heavy-ish things — protect your lean mass. (the surprising one)
Here’s the fix that isn’t about your feet at all. When you lose weight fast, you don’t only lose fat — you can lose muscle too, and less muscle can mean a softer, less “supported” look everywhere, feet included. Resistance training two to three times a week helps you hold onto lean mass, which improves body composition and how your skin and tissue sit over the frame. It won’t regrow a fat pad, but it changes the overall picture more than any foot cream will.
4. Eat enough protein.
Protein gives your body the raw material to preserve muscle and support skin repair during rapid loss. Under-eating protein while losing fast is a common, avoidable mistake — pharmacists and dietitians see it constantly in GLP-1 users whose appetite has cratered. If your appetite is low, prioritise protein first at every meal.
5. See a podiatrist when pain or skin problems persist.
If you have ongoing heel or arch pain, recurring blisters, or pressure sores, a podiatrist can assess your gait, prescribe proper orthotics, and rule out other causes. This is not a “wait and see” if you have diabetes — revisit the red-flag box above.
Two soft, honest notes on options. If you’re exploring or comparing treatments, you can browse GLP-1 and weight-loss medication options to see what the category includes. Separately, MedsBase lists a research-grade semaglutide product intended for laboratory research use only — that framing matters, and it should never be confused with a prescribed weight-loss treatment or self-dosed. Whatever route you consider, pace and professional guidance beat speed every time.
Related Reading
- Is the same thing happening to your face? — the sister phenomenon, explained.
- What happens if you stop taking Ozempic — including what changes may reverse.
- How to recognise a semaglutide overdose — because pacing and dosing safety go together.
The Sister Phenomena: Ozempic Face and Beyond
Your feet aren’t the only place the “same fat, faster than the skin can adapt” story plays out. The most famous version is Ozempic face — the hollowed, older-looking facial appearance some people develop when facial fat drops quickly. It’s the exact same mechanism as Ozempic feet: rapid volume loss plus lagging skin retraction, just somewhere more visible. If your feet changed, your face may be next on your list of questions, so it’s worth reading is the same thing happening to your face?
You’ll also hear about “Ozempic butt” and general loose skin on the arms and abdomen. Same root cause every time. Once you understand the mechanism in the feet, you understand it everywhere: the phenomenon follows the fat loss, and the fixes — pacing, strength, protein, patience — are broadly the same across the body. The face and feet just happen to be where people notice first.
Frequently Asked Questions
Does Ozempic make your feet smaller?
It can, indirectly. Ozempic feet often includes a half-size shoe drop because you lose fat (and sometimes fluid retention) around the foot. It’s not the drug shrinking your feet on purpose — it’s overall fat loss reducing foot volume. If your shoes now slip, re-measure; you may genuinely need a smaller size or better-fitting footwear.
Why do my feet hurt on Ozempic?
New foot pain during GLP-1 weight loss is often linked to thinner cushioning fat pads, which reduces shock absorption underfoot — thinner heel pads are associated with more heel pain in research. Supportive shoes and cushioned insoles usually help. If you have diabetes, do not assume it’s just cushioning — new pain, numbness, or non-healing sores need prompt medical review.
Can weight loss cause saggy skin on your feet?
Yes. When fat leaves faster than skin can retract, you can get loose or crepey skin, including on the tops of the feet and around the ankles. It’s more common with older skin, faster loss, and higher starting weight. It often softens over months as skin adapts, though very large losses sometimes don’t fully reverse without more time or professional input.
Is Ozempic feet permanent?
Not necessarily. Skin has some capacity to retract over months, and improving muscle mass and body composition helps the overall look. Fat pads may partly recover if weight stabilises, but very large or very fast losses can leave lasting changes. The honest answer: some of it improves with time and strength work; some may persist. There’s no guarantee either way.
Do you lose fat in your feet with GLP-1 medications?
You lose fat throughout the body, and the feet aren’t exempt — including the protective fat pads. You can’t spot-choose where fat comes off. This is why foot changes appear alongside changes in the face, arms, and abdomen. It reflects total-body fat loss, not a foot-specific drug effect.
How do I stop foot pain from rapid weight loss?
Start with footwear: cushioned, well-fitting shoes plus supportive insoles to replace lost padding. Add resistance training and adequate protein to protect lean mass, and pace your weight loss rather than chasing speed. If pain persists, see a podiatrist for a proper assessment — and if you have diabetes, seek care promptly rather than waiting.
Should I stop my medication because of Ozempic feet?
Cosmetic foot changes are rarely a reason to stop an effective, prescribed treatment — and stopping has its own consequences worth understanding first. Never adjust or stop a prescribed medication on your own; that’s a decision for you and your prescriber, weighing the benefits against the changes that bother you.
Medical Disclaimer
This article is for general information and education only and is not medical advice. It does not replace consultation with a qualified healthcare professional. Do not start, stop, or change any medication based on this content. If you have diabetes or any new or worsening foot symptoms, seek professional care promptly. Individual results and risks vary.
The Bottom Line
Here’s the balanced verdict. Ozempic feet is real, common, and almost always benign — it’s your feet losing cushioning fat and your skin lagging behind fast weight loss, not the medication attacking your feet. It shows up across every method of big, fast weight loss, because it follows the loss, not the drug. The changes tend to be milder with GLP-1 medications than after bariatric surgery, and pacing, footwear, strength training, and protein all help.
The one action to take today: if your shoes now slip, re-measure your feet and add a cushioned insole — a five-minute fix that prevents blisters and eases the “walking on hard floors” feeling. And if you have diabetes and any numbness, non-healing sores, or new foot pain, book that clinician visit now, not later. That single distinction — cosmetic versus diabetic — is the most important takeaway on this page.
Still mapping out your GLP-1 journey? Two natural next reads: what happens if you stop taking Ozempic, and — because side effects aren’t the only hidden risk in your medicine cabinet — another medication risk hiding in plain sight: grapefruit interactions. Your feet were just the first clue that fast weight loss changes more than the number on the scale.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.