







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
You drew up 50 units instead of 5. Or you injected today’s dose, then couldn’t remember whether you’d already done it this morning. Now you’re staring at your phone, heart pounding, typing “semaglutide overdose” and bracing for the worst. Take a breath — a semaglutide overdose is frightening, but for most people it is not the fast, catastrophic emergency that word suggests. It usually plays out slowly, as miserable nausea rather than sudden collapse.
This is not a reason to shrug it off, though. A 10× dose can leave you vomiting for days and drifting toward dehydration, and the risk profile changes if you also take insulin. So here’s the payoff: by the end of this guide you’ll know exactly what a semaglutide overdose does to the body, which symptoms mean “call for help right now,” the single number to dial first, and why a mistake made today can still be affecting you two weeks from now. One detail about the drug’s half-life surprises almost everyone — we’ll get to it in the timeline section.
Quick Answer: Accidentally taking too much semaglutide most often causes severe, prolonged nausea, vomiting, and abdominal pain rather than sudden life-threatening toxicity. The main dangers are dehydration and — if you also use insulin or a sulfonylurea — low blood sugar. There is no antidote; care is supportive. Call Poison Help at 1-800-222-1222 (US) or your local poison center right away, and go to the ER for persistent vomiting, confusion, fainting, or signs of severe low blood sugar.
Key Takeaways
- A semaglutide overdose rarely causes opioid-style acute lethal toxicity — but the “usually not fatal” reassurance comes with a real dehydration and low-blood-sugar catch.
- Most cases trace to one avoidable mix-up: milligrams vs milliliters vs “units” when drawing from a vial — the FDA has documented doses 5 to 20 times too high.
- Symptoms can last far longer than you’d expect — the reason is a number most people never think about.
- There’s no antidote. The right first move isn’t a home remedy — it’s a specific phone call we spell out below.
- One combination turns a “wait it out” situation into an emergency — knowing it in advance could matter.
- The format you inject from (pen, vial, or tablet) quietly decides how easy a dosing error is to make.
On this page
How Common Is a Semaglutide Overdose?
If you just made a dosing mistake, here’s something that may steady you: you are far from alone. As semaglutide moved from a diabetes drug to a widely used weight-management medicine, accidental exposures climbed sharply.
A 2026 analysis of U.S. poison-center data, published in the Journal of Medical Toxicology, found that reported GLP-1 exposures more than doubled after the weight-loss approval — from 3,113 cases in the pre-approval period to 6,920 afterward. Semaglutide alone made up about 64% of the later cases. The reassuring part: the researchers reported that most exposures were unintentional dosing or timing errors, and most symptoms were mild.
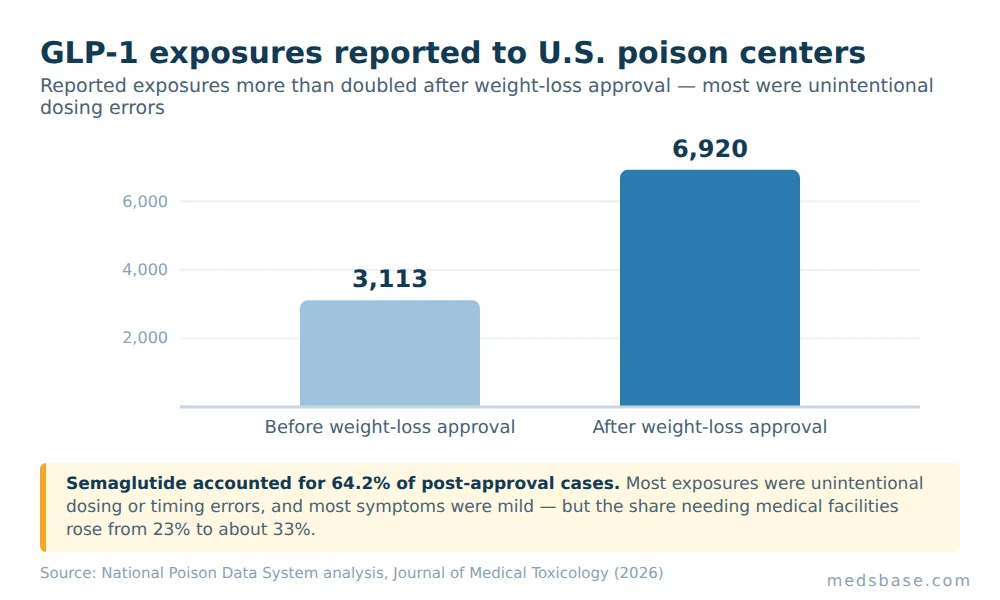
That said, the same data showed more people ending up in medical facilities — the share referred to or already at a hospital rose from 23% to about 33%. So these events are common, usually manageable, and occasionally serious enough to need care. That’s the honest middle ground this guide sits in.
Here’s what that means for you: a dosing mistake is a known, well-documented event that poison centers handle every day — which is exactly why calling one is the calm, normal response, not an overreaction.
What Counts as a Semaglutide Overdose?
A semaglutide overdose is any dose meaningfully higher than what was prescribed or intended for you — whether that’s a single large accidental injection, a double dose taken too close together, or a steadily-too-high dose from a miscalculation. Because semaglutide is dosed in small amounts and escalated slowly over weeks, even a modest error can represent several times your intended dose.
There’s no universal “toxic threshold” number that applies to everyone, and that’s an important honesty point. How a too much semaglutide situation plays out depends on the size of the excess, how far along your dose escalation you are, your hydration, and — critically — what other medicines you take. A person on the 0.25 mg starting dose who accidentally takes 2.5 mg is in a very different position from someone nudging slightly over their maintenance dose.
What the excess dose does not do is act like an opioid or a sedative overdose, where the danger is rapid and mechanical. Semaglutide has no known acute mechanism that shuts down breathing. The trouble it causes is mostly an exaggerated version of its ordinary side effects — turned up loud and stretched out over time.
Why Semaglutide Dosing Errors Happen — the mg/mL/Units Trap
Here’s where most of these stories actually begin — and it’s rarely carelessness. It’s a measurement trap.
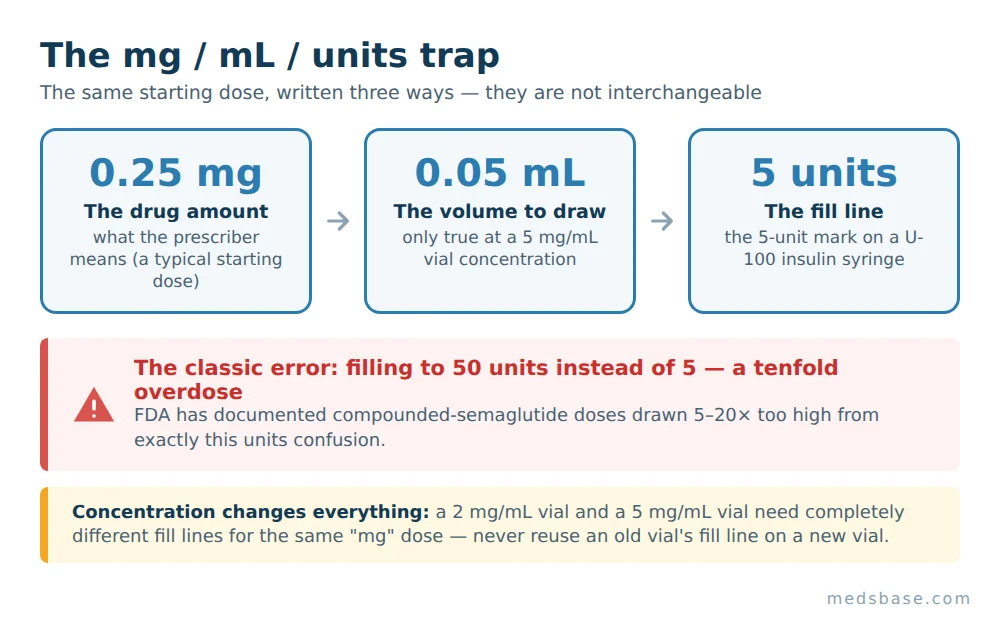
The prefilled branded pen does the math for you: you dial a dose, and mechanical stops prevent you from delivering wildly more. But compounded semaglutide often comes in a multiple-dose vial, and you draw it yourself with a syringe. Now three different units are in play at once — milligrams (the drug amount), milliliters (the volume), and “units” on the syringe barrel — and they are not interchangeable. That’s the heart of most every semaglutide dosing error.
The FDA’s alert on dosing errors with compounded injectable semaglutide (issued in 2024) documented exactly this. In many reports, patients drew up 5 to 20 times their intended dose. The classic case: a patient told to give “5 units” (0.05 mL) from a vial, using a U-100 insulin syringe, instead filled to 50 units — a tenfold overdose. The FDA also noted providers miscalculating conversions, prescribing 25 units when they meant 5, or 20 units when they meant 2.
Clinical insight: Pharmacists see this pattern constantly — a patient reads “units” on the syringe as if it were the dose, when the units only describe volume at a specific concentration. Two vials labelled the same “mg” can need completely different fill lines if their concentrations differ.
Here’s a worked example of how the same physical dose looks across the three units, so the trap is easy to see:
| What you’re told | What it means | On a U-100 insulin syringe | Common mistake |
|---|---|---|---|
| “Inject 0.25 mg” | The drug amount (a typical starting dose) | Depends entirely on vial concentration | Assuming “0.25” = 25 units |
| “That’s 0.05 mL” | The volume to draw | The 5-unit line | Reading the number 5 as 50 |
| “Draw to 5 units” | Volume marking on the barrel | Fifth small line | Filling to 50 (the tenfold error) |
| Concentration matters | 2 mg/mL vs 5 mg/mL vials need different volumes | Same “mg,” different fill line | Reusing an old vial’s fill line on a new, stronger vial |
If any row above made you go “wait, which one am I doing?” — that reaction is the risk, and it’s why double-checking in good light before every injection matters so much. For the correct escalation approach in the first place, our guide on how to read an Ozempic dosage chart the right way walks through the standard step-up schedule.
What Actually Happens in a Semaglutide Overdose
So you’ve taken too much. What should you expect your body to do?
Overwhelmingly, the answer is gastrointestinal misery, amplified. The FDA-approved Ozempic prescribing information notes that overdose in trials was chiefly associated with severe nausea and vomiting, and states plainly that there is no specific antidote — management is supportive care based on your symptoms. The FDA’s compounded-semaglutide reports listed nausea, vomiting, abdominal pain, fainting, headache, migraine, dehydration, and in some cases acute pancreatitis and gallstones. Some patients needed hospital care.
Let me be precise about the real dangers, because “just nausea” undersells them:
- Dehydration and electrolyte disturbance. Days of vomiting and poor fluid intake can drop your fluid volume and throw off potassium and sodium. In older adults or people with kidney issues, this is the failure point that lands someone in the ER — not the drug itself.
- Low blood sugar (hypoglycemia). On its own, semaglutide rarely causes dangerous lows. But combined with insulin or a sulfonylurea (like glipizide or glimepiride), a GLP-1 overdose can push blood sugar down hard. This is the one combination that turns “wait it out” into “watch closely and be ready to act.” (That was the open loop from the takeaways — this is the combination to know.)
- Aspiration and general depletion. Repeated vomiting risks dehydration, exhaustion, and, rarely, inhaling stomach contents.
The MedlinePlus page on semaglutide injection is a useful neutral reference for the drug’s ordinary side-effect list, which an overdose simply exaggerates.
Research Spotlight
Think of semaglutide’s effect like turning down a dimmer on your stomach and appetite signals. A normal dose lowers the lights gently. An overdose slams the dimmer to near-zero — your gut nearly stops moving, nausea floods in, and because the drug clears slowly, the room stays dark for a long time. That “slow clearance” is the detail almost everyone underestimates — and it’s next.
The One Detail That Catches Everyone Off Guard: the Half-Life
Here’s the part that surprises people. Semaglutide has a half-life of roughly one week. In plain terms, seven days after your dose, about half of it is still in your body — and it takes roughly five half-lives to mostly clear. That’s about five weeks.
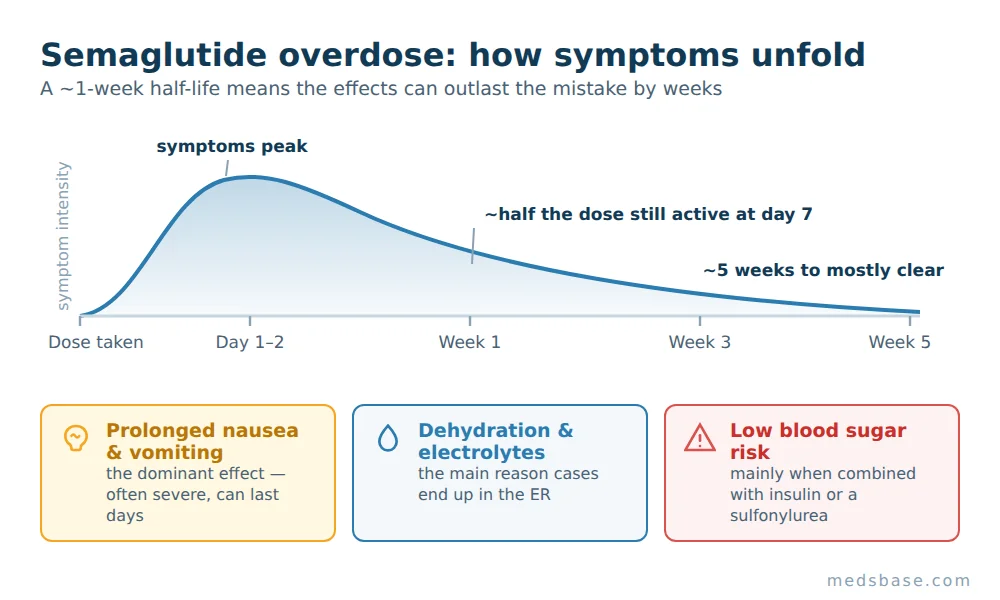
Practically, that means the effects of a single accidental semaglutide dose don’t peak and vanish in a day like a painkiller. Symptoms from a significant overdose can build over the first day or two and then linger — sometimes for a week or more of on-and-off nausea and appetite loss. The FDA label itself advises a prolonged period of observation and treatment after overdose, precisely because of this long half-life.
This is why “just ride it out at home” isn’t automatically the plan — a mistake made today may still need management next week, and that’s exactly the kind of judgement a poison center or clinician should help you make rather than guessing alone.
Red Flags: When a Semaglutide Overdose Is an Emergency
Most dosing errors are managed at home with fluids and rest — after you’ve checked in with a professional. But some signs mean stop reading and get help now. Use this table, then call.
| Sign / symptom | What it may mean | What to do |
|---|---|---|
| Vomiting you can’t stop; can’t keep any fluids down | Dehydration risk climbing | Call poison center; head to the ER if it continues |
| Confusion, slurred speech, shakiness, sweating, faintness | Possible severe low blood sugar (esp. if on insulin/sulfonylurea) | Treat low sugar if able; call emergency services |
| Severe, constant upper-abdominal pain radiating to the back | Possible pancreatitis | Emergency care now |
| Fainting, chest pain, trouble breathing | Serious systemic reaction | Call emergency services |
| Signs of dehydration: dizziness on standing, very little urine, racing heart | Fluid/electrolyte depletion | Contact poison center / seek care |
| No severe symptoms, but you know you overdosed | Needs a professional risk read given the long half-life | Call Poison Help 1-800-222-1222 for guidance |
Your first call, in almost every case, is the poison center — not the internet. In the US that’s Poison Help, 1-800-222-1222, free and confidential, 24/7. Outside the US, contact your local poison information center or emergency number. They will triage your specific dose, weight, and other medicines and tell you whether home monitoring or the ER is right. Whatever your symptoms, if you’re unsure or worsening, seek medical care rather than waiting.
The one-line takeaway: No proven antidote exists for a semaglutide overdose — which is exactly why fast professional triage, not a home fix, is the move that protects you.
Pen vs Vial vs Oral — Where Dosing Errors Actually Hide
Not every format carries the same risk. This is worth understanding, because it explains why some people almost can’t overdose by accident and others are one misread away from a tenfold error.
| Feature | Prefilled pen (branded) | Compounded vial + syringe | Oral tablet |
|---|---|---|---|
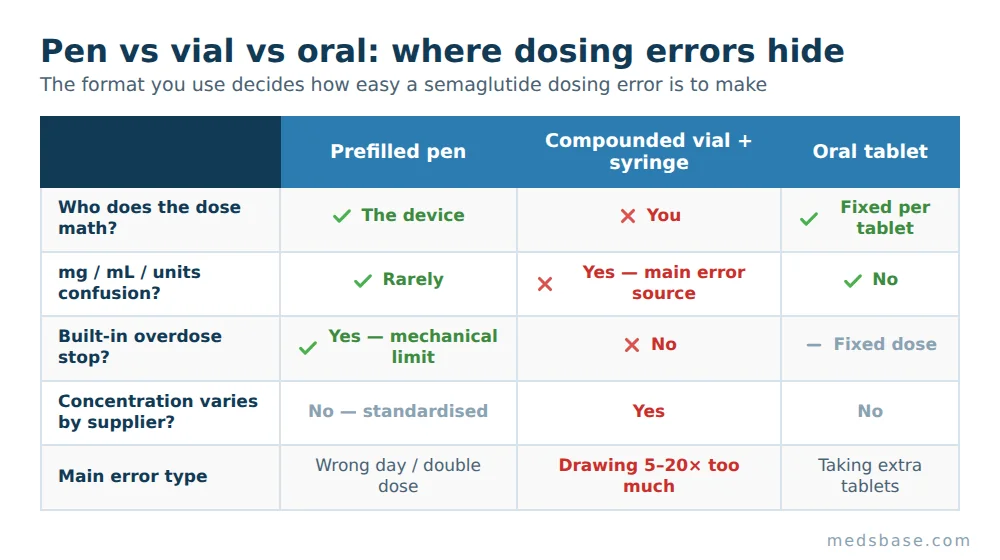
| Who does the dose math? | The device | You | The tablet (fixed) |
| mg vs mL vs units confusion possible? | Rarely — you dial a dose | Yes — the main error source | No |
| Built-in overdose stop? | Yes (mechanical dose limit) | No | Fixed per tablet |
| Concentration varies by supplier? | No (standardised) | Yes | No |
| Main error type | Wrong day / double dose | Drawing 5–20× too much | Taking extra tablets |
The verdict: the branded prefilled pen protects you most, because the dosing math and an overdose stop are built in — your realistic error is a forgotten or doubled dose. The compounded semaglutide vial gives flexibility and often lower cost, but it hands you the units math, and that’s where the serious 5–20× errors happen. A poison-control case series on compounded semaglutide administration errors documented exactly these vial-drawing mistakes. Oral semaglutide sidesteps injection math entirely, though it has strict fasting-timing rules of its own.
If you’re weighing formats, our explainer on how compounded semaglutide differs from the branded pen breaks down the trade-offs beyond just dosing safety.
Who This Matters Most For / Who Should Be Extra Careful
Most at risk of a dosing error: first-time self-injectors, anyone using a multiple-dose vial, people switching between vials of different concentrations, and those “catching up” after missed doses. Extra caution on the danger side: anyone also taking insulin or a sulfonylurea (hypoglycemia risk), older adults, and people with kidney disease (dehydration risk). If that’s you, keep the poison-center number saved before you ever need it.
What Does the Research Say?
Recency matters here, because this topic is in the news for a reason. Here’s a plain-language summary of the current evidence, with qualifying language throughout.
| Source | Year | Finding (as reported) | Reference |
|---|---|---|---|
| National Poison Data System analysis, J. Medical Toxicology | 2026 | GLP-1 exposures reported to U.S. poison centers more than doubled after weight-loss approval (3,113 → 6,920); semaglutide ~64% of later cases; most were unintentional errors | PubMed |
| Pediatric vs adult GLP-1 exposures, J. Medical Toxicology | 2026 | ~13,900 exposures 2017–2024; therapeutic errors ~86%; most had no or mild effects; vomiting far more common in symptomatic children | PMC |
| FDA safety communication (compounded semaglutide) | 2024 | Reports of 5–20× dosing errors from vial/units confusion; adverse events incl. nausea, vomiting, dehydration, some pancreatitis | FDA |
| Ozempic prescribing information (Overdosage) | 2025 | No specific antidote; supportive care; prolonged observation due to ~1-week half-life | FDA label |
What this means for you: the research consistently points the same direction — overdoses are common and usually driven by honest mistakes, symptoms are most often mild-to-moderate, but a rising share of people need medical care, and there’s no quick fix. The evidence base on rare severe outcomes is still limited, so treat any big overdose as a “get professional guidance” event rather than assuming the average outcome will be yours.
How to Prevent a Semaglutide Overdose
The best overdose is the one that never happens. If you use a vial and syringe, build these five habits — they close nearly every gap that leads to a semaglutide dosing error.
- Confirm the concentration first. Read the vial’s mg/mL every single time, especially with a new vial. A different concentration means a different fill line for the same dose. Reputable suppliers state concentration clearly — for example, MedsBase lists research-grade Semaglutide with the per-vial concentration stated on the product specifications; check that figure before you calculate anything.
- Match the syringe to the dose. Small doses need a small syringe. The FDA specifically flagged patients given syringes far larger than their dose — an oversized barrel makes the tenfold error easy. Ask your provider or pharmacist for the right syringe size.
- Do the mg → units conversion once, write it down, and post it. Don’t re-derive it half-asleep each morning. Tape the exact fill line to your fridge or medicine box.
- Double-check the fill line in good light, at eye level, before injecting. Ten seconds of looking prevents a week of vomiting. If the plunger looks “too full” versus your written note, stop and recheck.
- Never “catch up” a missed dose. If you miss one, do not add it to the next. Follow the standard schedule — our Ozempic dosage chart guide shows the correct step-up and what to do after a gap. And get your injection technique and site rotation right so nothing about the routine feels rushed or improvised.
Related Reading
- How to read an Ozempic dosage chart the right way — nail the correct escalation so you never have to “guess” a dose.
- Compounded semaglutide vs the branded pen — why the format you choose changes your error risk.
- Semaglutide injection sites: stomach, thigh, or arm — technique that keeps dosing calm and consistent.
Frequently Asked Questions
Can you overdose on semaglutide?
Yes — you can take more than intended, and it’s increasingly common as vial-based use grows. The good news is that a semaglutide overdose usually causes severe, prolonged nausea and vomiting rather than sudden life-threatening toxicity. The real risks are dehydration and, if you also use insulin or a sulfonylurea, low blood sugar. Contact Poison Help (1-800-222-1222 in the US) or your local poison center for personalised guidance.
What happens if you take too much semaglutide?
Expect an exaggerated version of the drug’s usual side effects: intense nausea, vomiting, abdominal pain, and appetite loss, sometimes with headache or faintness. Because semaglutide clears slowly, these can last days to weeks. Severe cases have involved dehydration and, rarely, pancreatitis. Watch for red-flag symptoms and seek medical care if you can’t keep fluids down or feel confused.
How much semaglutide is too much?
There’s no single toxic number that fits everyone — it depends on the size of the excess, where you are in dose escalation, and your other medicines. Because doses are small and escalated slowly, even a 5–10× error is significant. Rather than self-diagnose the severity, call your poison center with your exact dose and weight; they triage this daily.
How long do semaglutide overdose symptoms last?
Longer than most people expect. Semaglutide’s half-life is about one week, so symptoms from a significant overdose can build over a day or two and then linger for a week or more. The FDA label recommends a prolonged observation period for this reason. If symptoms persist or worsen at any point, don’t wait it out — seek medical advice.
Is a semaglutide overdose fatal?
Fatal outcomes from an isolated semaglutide overdose appear to be rare, and there’s no known rapid lethal mechanism like there is with opioids. But “rarely fatal” is not “harmless” — dehydration and low blood sugar (especially with insulin or a sulfonylurea) can become dangerous, and complications like pancreatitis do occur. Treat any large overdose as a reason to get professional guidance immediately.
I injected too much — should I skip my next dose?
Possibly, but that’s a decision to make with a professional, not alone, because the long half-life means the extra drug is still active. Do not take another dose to “reset,” and do not double up later. Call your poison center or prescriber; our guide on what happens when you stop taking Ozempic explains what pausing does, but let a clinician confirm your specific plan.
Is there an antidote for a semaglutide overdose?
No proven antidote exists. Treatment is supportive — managing nausea and vomiting, replacing fluids and electrolytes, and monitoring blood sugar — guided by your symptoms and how much you took. This is exactly why calling semaglutide poison control early matters: they help decide whether home monitoring or hospital care is appropriate.
The Bottom Line
Here’s the balanced verdict. A semaglutide overdose is usually a slow-burning problem, not an instant catastrophe — most cases mean days of rough nausea, not sudden danger. But that reassurance travels with two honest caveats: dehydration from relentless vomiting is real, and low blood sugar becomes a genuine threat if you also take insulin or a sulfonylurea. There’s no antidote, and the drug’s roughly one-week half-life means the effects can outlast the mistake by weeks.
Your one immediate action: if you (or someone with you) took too much, save and call Poison Help at 1-800-222-1222 (US) or your local poison center now — before searching for more reassurance. They’ll triage your exact situation calmly and tell you whether to monitor at home or go in. And if severe vomiting, confusion, fainting, or signs of low blood sugar appear, treat it as an emergency.
Once you’re through the scary part, prevention is mostly about the units math — confirm concentration, match your syringe, and never catch up a missed dose.
What to read next:
- Worried the mistake will affect your progress? See what happens when you stop taking Ozempic to understand pausing safely.
- Storing your vials or pens through a heat wave? A degraded, overheated dose adds potency uncertainty on top of dosing uncertainty — our companion guide on how to store medications in hot weather covers exactly that.
Medical Disclaimer
This article is for general education only and is not medical advice, diagnosis, or a substitute for professional care. It does not replace guidance from your doctor, pharmacist, or a poison-control specialist. If you suspect a semaglutide overdose, contact Poison Help (1-800-222-1222 in the US) or your local poison center immediately, and seek emergency care for severe or worsening symptoms. Never start, stop, or change a medication dose based on this page alone — decisions about dosing are individual and should be made with a qualified healthcare professional.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.