







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Picture this number: in a retrospective analysis of 5,638 women with a long history of urinary tract infections, starting vaginal estrogen for recurrent UTIs was linked to episodes falling from 3.9 to 1.8 per year — a drop of roughly 52%. That is not a supplement claim or a wellness trend. It comes from patient records reviewed and published in a peer-reviewed obstetrics journal, and this week the conversation grew louder because newer data suggests the benefit may reach beyond infection counts into fewer hospital stays.
If you or someone you love is stuck in the antibiotic-then-another-antibiotic cycle after menopause, this guide is for you. By the end, you’ll understand exactly how this treatment works, what the evidence does and does not prove, how the cream, tablet, and ring compare, and — just as importantly — who should talk to a doctor before starting. One detail about the safety history surprises almost everyone, and we’ll get to it in the safety section.
Key Takeaways
- A large records review linked vaginal estrogen to about 52% fewer recurrent UTIs — but the study design has one honest limit we’ll name.
- It works by fixing the cause, not masking symptoms — and the mechanism starts with a bacteria most people have never heard of.
- Low-dose vaginal estrogen behaves very differently from the estrogen pills that carried scary warnings — the reason is all about absorption.
- Cream, tablet, and ring each win for a different type of person — one costs the least, another is the easiest to forget.
- A history of breast cancer doesn’t automatically rule it out — but it does change who needs to be in the room for the decision.
On this page
What Is Vaginal Estrogen for Recurrent UTIs?
Vaginal estrogen for recurrent UTIs is a low-dose estrogen applied directly to the vaginal tissue — as a cream, tablet, insert, or ring — to rebuild the natural defenses that fade after menopause. Research suggests it lowers how often infections come back by restoring healthy tissue and a protective community of bacteria, rather than killing invaders like an antibiotic does.
Here’s the background. A urinary tract infection counts as “recurrent” when you have two or more in six months, or three or more in a year. After menopause, this pattern becomes far more common, and it isn’t bad luck. As estrogen levels fall, the tissues of the vagina and lower urinary tract thin, dry, and lose their acidity — a cluster of changes doctors now group under genitourinary syndrome of menopause (GSM).
That shift matters because your body’s front-line defense against postmenopausal urinary tract infections depends on estrogen. Take that hormone away locally, and the door is left open. Put a little back, right where it’s needed, and the door can close again.
This is not the same as swallowing hormone pills for hot flushes. Low-dose vaginal estrogen acts mainly where you place it, which is the whole point — and the reason its safety story is so different from the systemic-hormone headlines you may remember. We’ll unpack that difference in detail.
How Does Vaginal Estrogen Work Against Recurrent UTIs?
Think of your vagina as a walled garden. When estrogen is plentiful, the walls are thick, the soil is rich, and a friendly ground-cover of Lactobacillus crowds out weeds. After menopause, the walls thin and the friendly cover dies back — so weeds (uropathogens) take over the bare soil and spread toward the bladder.
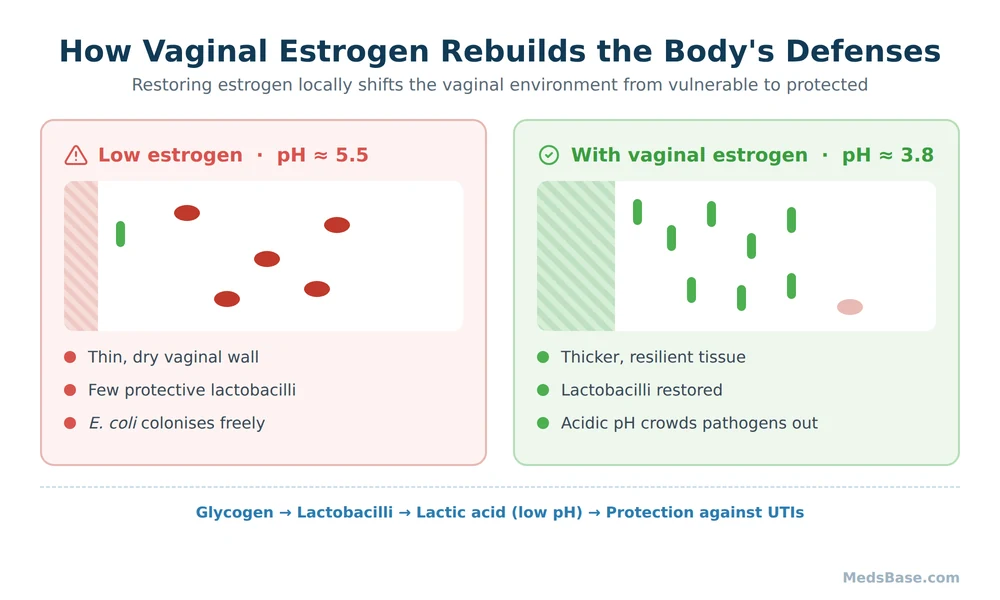
Vaginal estrogen therapy replants that garden. Within roughly two weeks of consistent use, the tissue thickens, glycogen returns, lactobacilli repopulate, and pH falls back into the protective range. A peer-reviewed review of how declining estrogen changes the vaginal microbiome describes several overlapping effects: estrogen thickens the epithelium, tightens the junctions between bladder-lining cells, and even boosts the tissue’s own antimicrobial peptides. So the benefit isn’t one mechanism — it’s a stack of them.
This is also why the effect isn’t instant. Antibiotics work in hours; recurrent UTI prevention with estrogen works over weeks, because you are rebuilding biology, not delivering a chemical strike.
Take Margaret, 68 (an illustrative example, not a real patient). She’d had five UTIs in a year and dreaded every twinge, convinced her body was simply failing her. What she hadn’t been told is that her infections weren’t random — they traced back to a single, correctable change: the loss of local estrogen and the protective bacteria that depend on it. Reframing “bad luck” as “a treatable cause” is often the moment the whole cycle starts to make sense. That is the shift good evidence makes possible, and it’s why understanding the mechanism matters as much as the prescription itself.
Research Spotlight: The 1993 Trial That Started It
In the landmark 1993 New England Journal of Medicine trial, postmenopausal women using intravaginal estriol saw UTIs fall to 0.5 episodes per patient-year versus 5.9 in the placebo group. Just as tellingly, protective Lactobacillus reappeared in 61% of treated women within a month — versus none on placebo — and vaginal pH dropped from 5.5 to 3.8. The mechanism and the outcome lined up perfectly.
One clarifying point on hormones: the estrogen in vaginal products is the same family of hormone as in menopause pills, but the dose and the destination are different. Wondering how local estrogen differs from systemic HRT? The short version: systemic HRT floods the whole body to treat hot flushes and bone loss; vaginal estrogen aims a tiny dose at the tissue that needs it. Same hormone, very different exposure.
Key Uses & Applications of Vaginal Estrogen
Preventing recurrent infections is the headline use, but it rarely travels alone. Because the underlying problem is GSM, one treatment often eases a whole set of overlapping symptoms.
Recurrent UTI prevention
This is the use with the strongest supporting data and the reason most women over 55 are offered it. It is considered a first-line preventive strategy for infection-prone postmenopausal women in specialist guidance.
Vaginal dryness and painful intercourse
The same tissue thickening that resists bacteria also relieves the dryness, irritation, and pain with sex that so often accompany menopause. Many women notice these improve before they even track their UTI count.
Urinary urgency, frequency, and mild leakage
Healthier bladder-neck and urethral tissue can reduce that “always needing to go” feeling. It is not a fix for every bladder problem, but for GSM-driven symptoms it often helps.
GSM symptom relief overall
Restoring the local estrogen environment addresses the cluster — dryness, thinning, pH, and infection risk — at the source rather than one symptom at a time.
Who Is This For? / Who Should Avoid It?
Likely a good fit if you are: postmenopausal (or otherwise low in estrogen — for example after certain cancer treatments, with a specialist’s guidance), stuck in a recurrent-UTI cycle, and want to reduce repeated antibiotic courses.
Pause and speak to a doctor first if you have: a personal history of breast or other hormone-sensitive cancer (this needs an oncologist conversation, not an automatic “no”), any undiagnosed vaginal bleeding, a history of blood clots or stroke, or known liver disease. Undiagnosed bleeding always needs investigation before any estrogen. When decisions are this individual, a clinician should help you weigh them.
Once a clinician agrees it fits, the cream format is the most familiar starting point. MedsBase stocks a conjugated-estrogens vaginal cream if you want to see options for Premarin conjugated-estrogens vaginal cream and compare formats — no prescription needed to browse. We’ll cover how the cream, tablet, and ring differ in practice shortly.
Vaginal Estrogen Safety Profile, Side Effects & Dosage
Now for the detail that surprises almost everyone — the open loop from the introduction.
Many women were told years ago that “estrogen causes cancer and clots,” and that message stuck. It came from large trials of systemic hormone therapy — estrogen taken as pills or patches that circulate through the whole body — where certain risks led to prominent boxed warnings. Those findings were real for systemic use.
Here’s the twist: low-dose vaginal estrogen delivers only a small fraction of that systemic exposure. Because you apply a tiny amount directly to the tissue, blood levels stay far lower than with oral hormones. That is why major professional bodies treat local vaginal estrogen as a distinct, lower-risk option — while still, appropriately, carrying the class labelling. The MedlinePlus estrogen (vaginal) drug information page lays out both the reassurances and the genuine cautions.
To be clear and not to minimise: the product labels still list the estrogen-class warnings, and that is why the “who should avoid it” box above matters. Association is not a guarantee of safety for every individual — your own history decides your risk.
| Side effect | Frequency | Severity | What to do |
|---|---|---|---|
| Local irritation, itching, or discharge | Common, early | Mild | Usually settles in 1–2 weeks; tell your prescriber if it persists |
| Mild breast tenderness | Uncommon | Mild | Often fades; mention it at review |
| Spotting or vaginal bleeding | Uncommon | Needs review | Stop and contact a doctor — any postmenopausal bleeding must be checked |
| Headache | Uncommon | Mild–moderate | Monitor; seek advice if severe or new |
| Signs of a clot (leg pain/swelling, sudden breathlessness, chest pain) | Rare | Urgent | Seek emergency care immediately |
Typical dosing pattern (always follow your own prescription): creams and tablets are often used nightly for the first 1–2 weeks to build tissue up, then dropped to about twice weekly for maintenance. The ring is replaced roughly every three months. The vaginal estrogen cream dose is measured with an applicator, and less is genuinely more here — the goal is local effect, not systemic levels.
Clinical insight: pharmacists commonly see two mistakes. The first is stopping after a couple of good weeks, which lets the tissue — and the infections — relapse. The second is doubling up “to work faster,” which only raises side-effect risk without speeding the biology. Consistency at the right dose beats intensity every time.
What Does the Research Say About Vaginal Estrogen for Recurrent UTIs?
The evidence sits on two legs: an old, high-quality randomized trial and newer, large real-world reviews. Together they tell a consistent story, though each has limits worth naming.
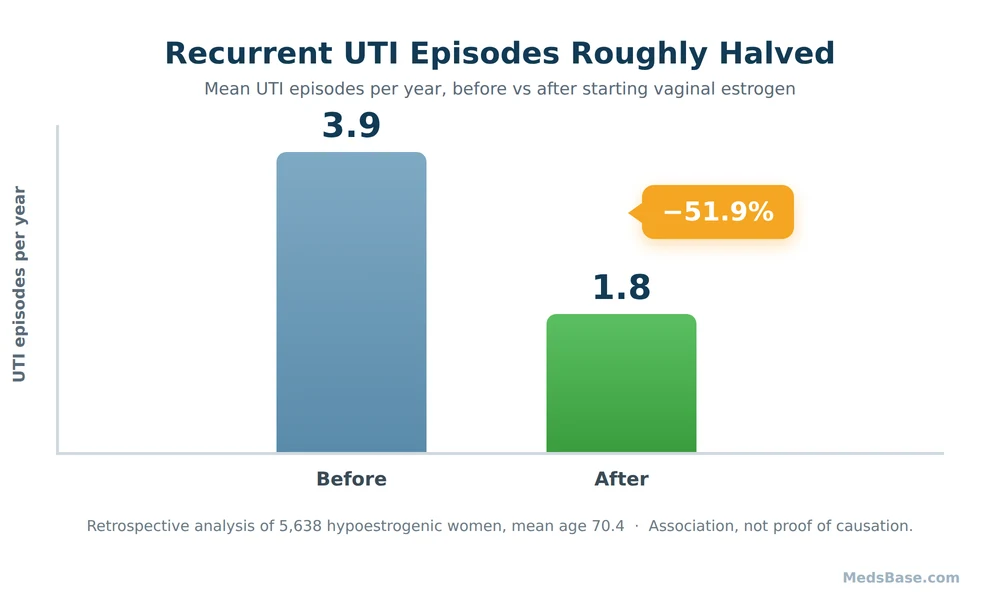
The chart shows mean recurrent UTI episodes per year falling from 3.9 before treatment to 1.8 after — a 51.9% reduction — in a retrospective review of 5,638 hypoestrogenic women (mean age 70.4).
| Study | Year | Finding | Source |
|---|---|---|---|
| Raz & Stamm, NEJM randomized trial of intravaginal estriol | 1993 | UTIs fell to 0.5 vs 5.9 episodes/patient-year; lactobacilli restored; pH normalised | PubMed 8350884 |
| Retrospective review, 5,638 hypoestrogenic women (mean age 70.4) | 2023 | Recurrent UTI episodes fell 3.9 → 1.8 per year (−51.9%); 31.4% had zero UTIs in follow-up | PubMed 37178856 |
| Mechanism review — estrogen, the epithelium & the microbiome | 2019 | Estrogen thickens tissue, tightens cell junctions, restores lactobacilli and antimicrobial peptides | PMC6376984 |
| Newer large analysis — serious outcomes (hospitalization, sepsis, mortality) | 2026 | Vaginal estrogen use reported as associated with lower hospitalization, sepsis, and all-cause mortality in women over 55 with recurrent UTIs | Preliminary 2026 analysis (peer-reviewed publication pending) |
What this means for you: the 1993 trial is randomized — the gold standard — and shows a clear cause-and-effect signal, but it was small. The 2023 review is large and real-world, which is powerful, but it is retrospective and observational: it shows a strong association, not proof, and the authors even flagged a counter-intuitive adherence pattern they attributed to unmeasured confounding. The newest serious-outcomes data is exciting precisely because it hints the benefit extends to hospital stays and sepsis — but until the specific analysis is peer-reviewed and published, treat those numbers as promising, not settled. Honest summary: strong, consistent evidence for fewer infections; encouraging early signals for bigger outcomes.
Why does the direction of the evidence matter so much for a decision like yours? Because recurrent infections in older women aren’t only uncomfortable — repeated antibiotic courses drive resistance, and in frail patients a UTI that climbs to the kidneys or bloodstream can turn serious quickly. A prevention strategy that reduces the number of infections is valuable on its own; one that might also reduce the worst outcomes would matter even more. That is exactly why researchers are now looking past episode counts toward hospitalization and sepsis. It is also why no honest guide should oversell a retrospective signal before it’s confirmed — the responsible read is cautious optimism, paired with a real conversation with your own clinician about your own risk.
Vaginal Estrogen vs Alternatives for Recurrent UTI Prevention
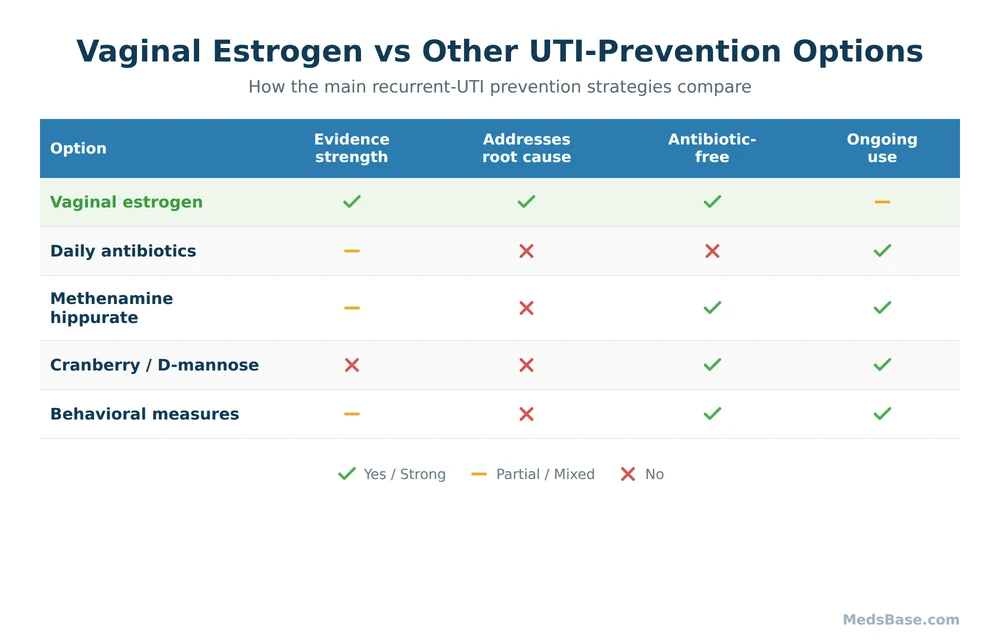
Estrogen isn’t the only tool for recurrent UTI prevention, and it isn’t right for everyone. Here’s how the main options compare.
| Option | How it works | Evidence strength | Best for | Main downside |
|---|---|---|---|---|
| Vaginal estrogen | Restores tissue, pH, and protective bacteria (fixes the root cause in GSM) | Strong for postmenopausal women | Postmenopausal, infection-prone, wants to reduce antibiotics | Not for undiagnosed bleeding; needs an oncologist chat after breast cancer |
| Daily prophylactic antibiotics | Continuously suppress bacteria | Effective but declines over time | Short-term bridge, or when estrogen isn’t suitable | Resistance, gut/vaginal microbiome disruption, side effects |
| Methenamine hippurate | Converts to formaldehyde in acidic urine, a non-antibiotic antiseptic | Growing; a useful antibiotic-sparing option | Those wanting to avoid daily antibiotics | Needs acidic urine; not for kidney/liver impairment |
| Cranberry / D-mannose | May reduce bacterial adhesion to the bladder wall | Mixed and modest | Low-risk add-on for the motivated | Inconsistent results; not a standalone fix for frequent recurrences |
| Behavioral measures | Hydration, voiding habits, wiping technique, post-sex urination | Sensible foundation, modest alone | Everyone, as a baseline | Rarely enough by itself in true recurrence |
Which one fits which situation? If you’re postmenopausal and infections keep returning, vaginal estrogen treats the actual cause and is favoured in specialist guidance such as the AUA/CUA/SUFU recurrent UTI guideline. If estrogen isn’t suitable, methenamine hippurate is the leading antibiotic-sparing alternative. Cranberry, D-mannose, and behavioral steps are reasonable companions — not replacements — for someone with a genuine recurrent pattern. Curious what actually helps between prescriptions? Our behavioral-measures guide covers the day-to-day habits.
How to Use Vaginal Estrogen — Practical Guidance
Getting the routine right is most of the battle. Here is the pattern most prescribers describe (yours may differ — follow your own instructions).
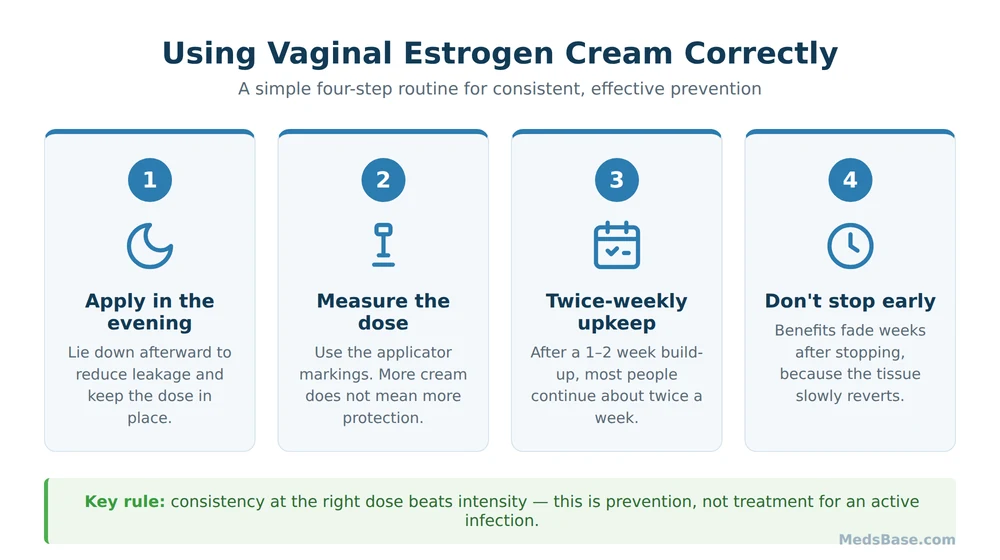
- Start with a build-up phase. Creams and tablets are often used nightly for the first one to two weeks so the tissue can thicken before you drop to maintenance.
- Apply in the evening. Lying down afterward reduces leakage and improves contact time, so the dose stays where it works.
- Move to twice-weekly maintenance. Once tissue is restored, most people continue about twice a week indefinitely. The ring is simply replaced roughly every three months.
- Measure the cream — don’t eyeball it. Use the applicator markings. More cream doesn’t mean more protection; it just raises side-effect risk.
- Don’t stop when you feel better. This is the single biggest mistake. Benefits fade weeks after you stop, because the tissue slowly reverts.
Mistakes to avoid:
- Quitting after two good weeks (relapse follows).
- Doubling the dose “to speed things up.”
- Ignoring new spotting instead of reporting it.
- Assuming it replaces treatment for an active infection — it’s for prevention, not for treating a UTI you have right now.
If your clinician has agreed the cream format suits you, you can check availability and strengths and compare it with other local-estrogen formats. No prescription needed to look, and soft is the whole tone here — this is a decision to make with a professional, not a rushed cart.
Related Reading
- How does local estrogen differ from systemic HRT? — the systemic-vs-local question, answered in full.
- What actually helps between prescriptions? — practical, evidence-aware UTI self-care.
- Explore the women’s health range — related products and categories in one place.
Frequently Asked Questions
Does vaginal estrogen prevent UTIs?
Research suggests it does for many postmenopausal women. A randomized 1993 trial found far fewer infections on intravaginal estriol than placebo, and a 2023 review of 5,638 women linked it to about 52% fewer recurrent episodes. It works by restoring protective tissue and bacteria, so it reduces recurrence rather than treating an active infection.
How long does vaginal estrogen take to work for UTIs?
Expect weeks, not hours. Tissue changes and Lactobacillus recovery begin within roughly two weeks of consistent use, and full preventive benefit builds over one to three months. This is biology being rebuilt, not a fast antibiotic strike — which is exactly why stopping early lets the problem return.
Is vaginal estrogen safe after breast cancer?
Not an automatic yes or no. Because breast cancer can be hormone-sensitive, this decision needs an oncologist’s input, weighing your cancer type, treatment, and symptom severity against the very low systemic absorption of local estrogen. Some women use it safely with specialist oversight; others are advised against it. The key is a conversation, not a guess.
Vaginal estrogen cream vs tablet vs ring — which is best for UTIs?
All three deliver low-dose local estrogen effectively; the choice is about lifestyle. Cream is flexible and often lowest cost but can be messier. Tablets and inserts are tidy and pre-measured. The ring is the easiest to forget in a good way — inserted and replaced about every three months. Effectiveness is broadly similar; convenience differs.
What are the side effects of vaginal estrogen?
Most are mild and local — irritation, itching, or discharge in the first couple of weeks, occasionally mild breast tenderness or headache. The important rule: any new vaginal bleeding or spotting should be reported to a doctor promptly, and clot warning signs need urgent care. Serious effects are rare with low-dose local use, but the estrogen-class cautions still apply.
Can you use vaginal estrogen with a history of blood clots?
This needs individual medical advice. Systemic estrogen raises clot risk, and while local vaginal estrogen exposes the body to far less hormone, a personal or strong family history of clots is a reason to discuss it carefully with your doctor before starting rather than deciding alone.
Do you need a prescription, and can you keep using it long term?
Clinically it’s commonly prescribed, and many women use it long term for ongoing prevention — the benefit lasts only while you keep using it. On MedsBase, no prescription is needed to browse options, but the decision to start and to continue is one to make with a clinician who knows your history.
Medical Disclaimer
This article is for general education and is not a substitute for personalised medical advice. Vaginal estrogen is a hormone treatment with genuine benefits and real cautions; whether it’s right for you depends on your individual history. Do not start, stop, or change any medication without speaking to a qualified doctor or pharmacist, and seek prompt care for any undiagnosed vaginal bleeding or signs of a blood clot.
The Bottom Line
The verdict on vaginal estrogen for recurrent UTIs is refreshingly clear for a health topic: for many postmenopausal women stuck in the antibiotic loop, it treats the actual cause and, across a randomized trial and a large real-world review, is consistently linked to substantially fewer infections — with encouraging new signals it may also reduce hospitalizations and sepsis. The honesty that earns your trust: the biggest study is observational, so it shows strong association, not ironclad proof, and it isn’t right for everyone.
Your immediate action: if you’ve had two or more UTIs in six months (or three in a year) and you’re postmenopausal, write that number down and ask your doctor or pharmacist directly whether low-dose vaginal estrogen fits your history. That one question reframes the whole cycle from “bad luck” to “treatable cause.”
Wondering whether the estrogen in these products is the same as menopause pills? Read how local estrogen differs from systemic HRT. And if you’re weighing antibiotics for prevention, know that several of them make your skin burn faster in the sun — worth checking before summer. You can also explore the women’s health range when you’re ready to compare options with your clinician.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.