







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Picture this. It’s the first real Saturday of the heat wave, and you spend three easy hours at the beach — nothing extreme, the same sun everyone around you is soaking up. By evening your shoulders and the tops of your feet are scarlet, stinging, and starting to blister. Your friends, out just as long, are barely pink. The difference? Two days ago your doctor started you on doxycycline for a chest infection. That is not ordinary bad luck. That is drug-induced photosensitivity, and it explains a burn that makes no sense for the sun you actually got.
Medications that cause sun sensitivity are more common than most people realise — and the reaction can look far worse than a normal sunburn. This guide gives you the full checklist the shallow “top 5 drugs” articles leave out: the 12 drug classes to watch, why the reaction happens (in plain English), how to tell it apart from simple heat intolerance, and exactly what to do — without ever stopping a medication on your own. By the end you’ll be able to scan your own medicine cabinet with confidence.
One detail surprises almost everyone: the sunscreen most people already own may be doing only half the job for this specific problem. We’ll get to why in the protection section.
Key Takeaways
- A dozen everyday drug classes can turn normal sun into an outsized burn — antibiotics are only the most famous; several are in most family medicine cabinets.
- Two very different reactions hide under one word — phototoxic (fast, common, looks like sunburn) and photoallergic (rare, delayed, looks like eczema). Knowing which you have changes what you do.
- The trigger is mostly UVA — the wavelength ordinary sunscreen often under-blocks. That single fact reshapes how you protect yourself.
- Heat intolerance is a separate July hazard. Some drugs stop you sweating properly rather than burning your skin — different mechanism, same season.
- The safest fix is almost never “stop the drug.” For heart and blood-pressure medicines especially, the move is a prescriber conversation about sun-safer alternatives.
On this page
What Are Medications That Cause Sun Sensitivity?
Medications that cause sun sensitivity are drugs that make your skin react abnormally to ultraviolet light, so a modest amount of sun triggers a burn, rash, or blistering far out of proportion to your exposure. Doctors call this drug-induced photosensitivity. It can start within hours of your first sunny day on the medicine, and it affects people who normally tan without trouble.
The mechanism is not “the drug makes you burn faster” in a vague sense. The medication (or a breakdown product of it) sits in your skin and absorbs UV energy, then unloads that energy into surrounding cells. The result ranges from an exaggerated sunburn to a spreading, itchy eruption. According to the FDA’s consumer guidance “The Sun and Your Medicine”, both prescription and over-the-counter products — from certain antibiotics to some pain relievers and diuretics — carry this potential.
Here’s the reassuring part, and the reason this guide exists: once you know your drug is on the list, the problem is highly manageable. You don’t usually have to choose between your treatment and the outdoors. You have to protect the right way and, where it matters, ask about a sun-safer option. The rest of this article shows you how.
How Does Drug-Induced Photosensitivity Work?
Think of a photosensitizing drug as a tiny antenna that has slipped into your skin. On its own it does nothing. Add ultraviolet light — specifically UVA, the longer-wavelength band that passes through clouds and window glass — and the antenna absorbs that energy and can’t hold it. It dumps the energy into nearby skin cells, and that’s where the damage begins.
That antenna analogy maps onto two genuinely different reactions. Getting the difference right is the single most useful thing on this page, because they look different, arrive on different timelines, and are managed differently.
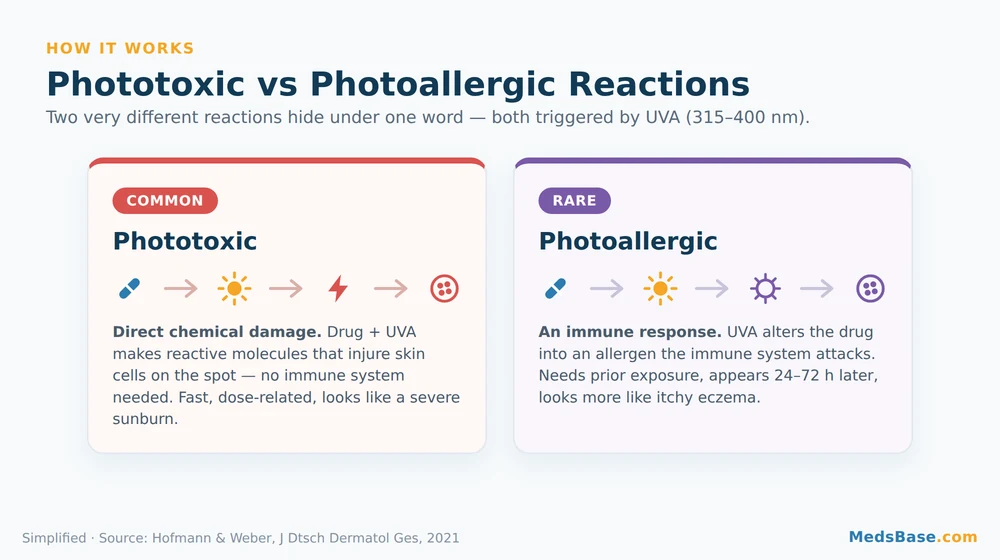
Phototoxic Reactions: the Common One
A phototoxic reaction is direct chemical damage. The drug plus UVA generates reactive molecules that injure skin cells on the spot — no immune system required. That’s why it can happen the very first time you take the drug and step into the sun, why it’s dose-related, and why it looks and feels exactly like a severe, sometimes blistering sunburn confined to sun-exposed skin. This is by far the more common of the two.
Photoallergic Reactions: the Rare One
A photoallergic reaction is an immune response. UVA changes the drug’s structure just enough that your immune system treats it as a foreign invader. This needs prior sensitisation, so it usually shows up after you’ve been on the drug a while, appears 24–72 hours after sun exposure, and looks more like eczema — itchy, bumpy, sometimes spreading slightly beyond the sun-exposed zone. It’s genuinely uncommon.
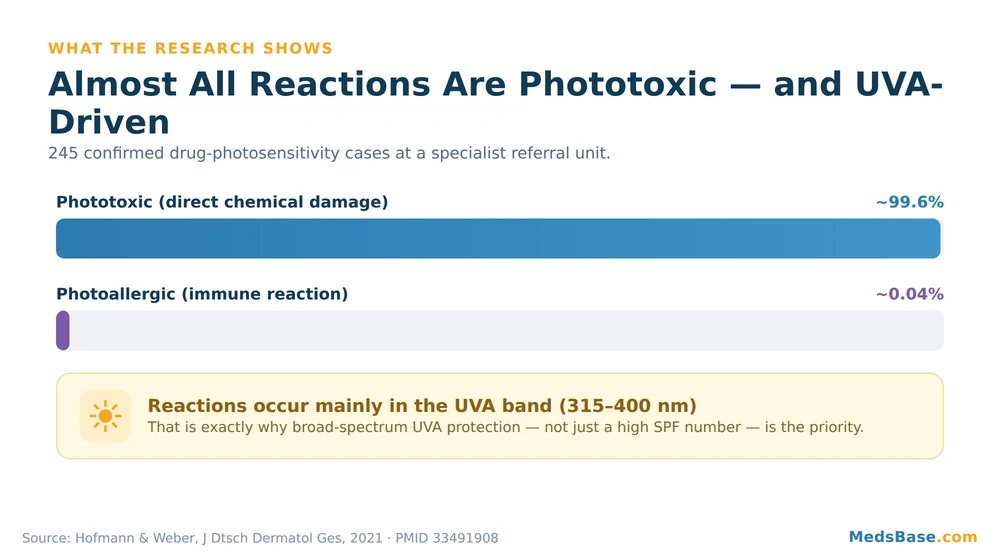
Research Spotlight
In a landmark analysis from a specialist photobiology unit spanning three decades, out of 245 confirmed drug-induced photosensitivity cases, just one was a true photoallergy — roughly 0.04%. The overwhelming majority were phototoxic. The same body of work notes reactions occur mainly in the UVA range (315–400 nm), which is why UVA protection matters so much. Source: a 2021 dermatology review of culprit drugs and mechanisms (Hofmann & Weber).
So what does this mean for you? If you develop a burn-like reaction fast, you’re almost certainly dealing with phototoxicity — the version that responds beautifully to UVA-focused protection. Keep that word, UVA, in mind; it’s the hero of the protection section later. And remember the open loop from the intro about your sunscreen — this is why it matters.
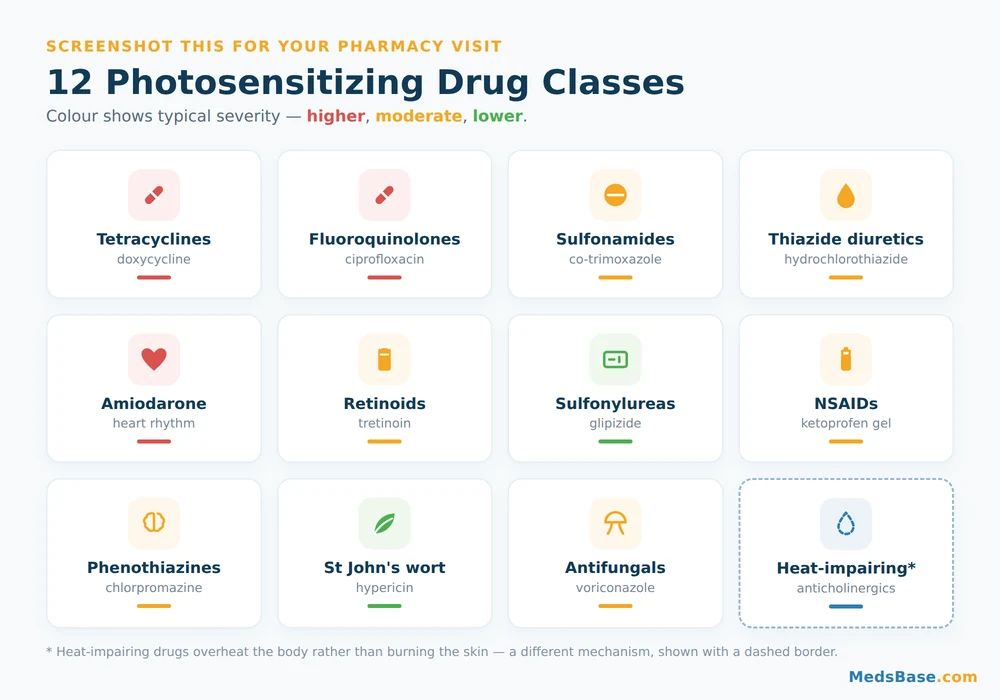
The 12 Drug Classes That Cause Sun Sensitivity
Most competing articles stop at five or six drugs. Here is the fuller landscape. The table below groups the well-documented photosensitizing drugs by class, with the reaction type usually seen, typical severity, how fast it appears, and — the part nobody else includes — what to actually do. Severity and onset are general patterns, not guarantees; individuals vary.
| Drug class (common examples) | Usual reaction type | Typical severity | Typical onset | What to do |
|---|---|---|---|---|
| Tetracyclines — doxycycline, minocycline, tetracycline | Phototoxic | Moderate–high (doxycycline notably so) | Hours to 1–2 days | Rigorous UVA sunscreen + cover-up; ask pharmacist about timing/alternatives |
| Fluoroquinolones — ciprofloxacin, levofloxacin, lomefloxacin | Phototoxic | Moderate | Hours to days | Avoid peak sun; UVA protection; report severe reactions |
| Sulfonamides / TMP-SMX — co-trimoxazole (Bactrim) | Phototoxic ± photoallergic | Moderate | 1–3 days | Cover exposed skin; flag any spreading rash to prescriber |
| Thiazide diuretics — hydrochlorothiazide, and related BP agents | Phototoxic (sometimes chronic/lichenoid) | Low–moderate, but persistent | Days; can build over weeks | Never stop on your own — ask about a sun-safer antihypertensive |
| Amiodarone (heart rhythm) | Phototoxic; blue-grey skin with long use | Moderate–high | Weeks–months | Strict sun avoidance; prescriber-managed only — do not self-adjust |
| Retinoids — tretinoin, isotretinoin, acitretin | Phototoxic + thinner, more vulnerable skin | Moderate | Days–weeks | Daily broad-spectrum sunscreen; see the retinoid deep-dive below |
| Sulfonylureas — glipizide, glimepiride, glibenclamide | Photoallergic-leaning | Low–moderate | Days | Sun protection; report rash; prescriber decides on changes |
| NSAIDs — ketoprofen (esp. gel), piroxicam, naproxen | Phototoxic + photoallergic (ketoprofen) | Moderate; ketoprofen gel can be marked | Hours–days | Wash off topical gel before sun; cover treated skin |
| Phenothiazines — chlorpromazine, prochlorperazine | Phototoxic + photoallergic | Moderate | Days | Sun protection; prescriber review if reaction occurs |
| St John’s wort (herbal, hypericin) | Phototoxic | Low–moderate, dose-related | Days | Treat like a drug; disclose to pharmacist; protect skin |
| Certain antifungals — griseofulvin, voriconazole (long-term) | Phototoxic | Moderate; voriconazole significant long-term | Days–weeks | Diligent protection; prescriber-monitored |
| Some antihistamines & others — e.g. promethazine, plus select chemo agents | Variable | Low–moderate | Variable | Read the leaflet’s sun warning; protect accordingly |
That’s roughly a dozen families — and notice how ordinary most of them are. A blood-pressure pill, a course of antibiotics, an acne cream, a herbal supplement from the health shop. You don’t have to be on anything exotic to be affected.
Antibiotics: the Class Most People Meet First
If you take away one name, make it doxycycline sun sensitivity. Tetracyclines — doxycycline above all — are the antibiotics most reliably linked to phototoxic burns, which is exactly why our hypothetical beachgoer at the top got scorched. MedlinePlus notes doxycycline can make skin sensitive to sunlight, and the NHS doxycycline medicine page gives the same warning to the public. This is well-established, not fringe.
If you’re taking doxycycline — commonly prescribed for chest and skin infections, acne, and some travel-related conditions — you can see doxycycline capsule options to check strengths, but the more important move is behavioural: treat your first sunny days on it with real caution. Fluoroquinolones (like ciprofloxacin) and the sulfonamide combination co-trimoxazole belong on the same watch-list, which matters because those two also treat urinary infections — a thread we’ll pick up at the end.
Who Should Read This Most Carefully — and Who Can Relax a Little
Pay close attention if you: are starting a tetracycline, fluoroquinolone, or sulfonamide antibiotic; take a thiazide diuretic or amiodarone; use a retinoid; are fair-skinned or burn easily; are heading somewhere sunny or into a heat wave.
You can worry less if you: are on a medication with no sun warning on the leaflet, stay well covered, or are simply reviewing your cabinet as a precaution. Not every drug photosensitizes — the goal is to know which of yours do, not to fear all of them.
Blood-Pressure and Heart Medications: the Quiet Entries
People expect antibiotics to cause sun sensitivity from antibiotics, but they’re blindsided by their heart and blood-pressure pills. Thiazide diuretics such as hydrochlorothiazide are among the most frequently documented photosensitizers, and amiodarone can even leave a blue-grey discolouration on chronically sun-exposed skin. Because these medicines protect against strokes and dangerous rhythms, the rule here is absolute: never stop or skip a heart medication because of the sun. Instead, if you react, ask your prescriber whether a sun-safer antihypertensive fits your situation — you can see heart & blood-pressure medication options to understand the range before that conversation.
Retinoids and Acne Treatments
Retinoids like tretinoin and isotretinoin both photosensitize and thin the skin’s outer layer, leaving it more vulnerable to UV. If this is your situation, we’ve written a dedicated companion piece on exactly how tretinoin and sun exposure interact — this umbrella guide points you there rather than repeating it. You can also explore acne treatment options if you’re weighing routines that fit a sunny climate.
Medications and Sun Sensitivity: Symptoms, Severity & What To Do
Time to resolve the loop we opened at the start — how bad can this get, and how do you tell a drug reaction from a plain sunburn? The honest answer: symptoms range from trivial to genuinely serious, and the tell-tale sign is proportion. A reaction that outstrips your actual sun exposure, or that appears on a drug with a known sun warning, points to photosensitivity.
Here’s what a phototoxic reaction looks like versus its milder and rarer cousins, with the practical response for each.
| Symptom / sign | How often | Severity | What to do |
|---|---|---|---|
| Exaggerated “sunburn” — redness, heat, stinging on sun-exposed skin | Common (phototoxic) | Mild–severe | Get out of the sun, cool the skin, hydrate; if blistering or widespread, seek medical care |
| Blistering, swelling, skin peeling | Occasional | Moderate–severe | Treat like a burn; medical review if extensive, on the face, or with fever |
| Itchy, eczema-like rash 1–3 days after sun | Uncommon (photoallergic) | Mild–moderate | Note the delay; tell your prescriber — it may spread beyond sun-exposed skin |
| Exaggerated response only where a topical gel was applied | Occasional (e.g. ketoprofen gel) | Moderate | Wash off before sun; cover the treated area |
| Blue-grey skin discolouration (chronic) | Rare (amiodarone, long-term) | Cosmetic but persistent | Prescriber-managed; do not self-adjust the drug |
| Darkened nails or a “false tan” look | Rare | Cosmetic | Usually reversible; mention at your next review |
When to get help promptly: blistering over a large area, facial swelling, signs of infection, fever, or any reaction that frightens you. Pharmacists commonly see people dismiss a drug reaction as “just a bad burn” and delay care — when in doubt, ask. A quick pharmacy conversation costs you nothing and can save a miserable week.
Crucially, treating the skin is only half the response. The other half is not repeating the exposure — which brings us to a hazard people confuse with photosensitivity but that works in a completely different way.
The July Twist: Heat Intolerance vs Photosensitivity
Not every summer medication problem is about sunlight hitting your skin. Some drugs make it harder for your body to cool itself — a distinct danger during a heat wave that has nothing to do with UV. This is heat intolerance from medications, and mixing it up with photosensitivity can leave you protecting the wrong thing.
The difference is mechanism. Photosensitivity is a skin reaction to light. Heat intolerance is a whole-body problem with temperature: certain medicines blunt sweating, reduce thirst signals, or affect blood flow and fluid balance, so your natural cooling system underperforms when it’s hot.
Drugs that can impair heat regulation include anticholinergics (some bladder, allergy, and gut medicines), many antidepressants and antipsychotics, stimulants, and diuretics (which shift fluid balance). Public-health bodies flag exactly these classes in hot-weather guidance for clinicians.
If you’re on a sweat-impairing medication, the summer priorities are shade, cool environments, hydration, and recognising early overheating (dizziness, nausea, confusion, a headache that won’t lift) — not just sunscreen. And, as always, you manage this with your prescriber, never by quietly skipping doses in the heat.
What Does the Research Say?
The evidence base for drug-induced photosensitivity is deeper than the thin listicles suggest. Here’s a compact summary of what reputable sources establish, with qualifying language where the science is still settling.
| Finding | Year | What it tells us | Source |
|---|---|---|---|
| Of 245 confirmed cases at a specialist unit, only ~0.04% were true photoallergy | 2021 review (data 1970–2000) | Phototoxic reactions dominate overwhelmingly | PMC review / PMID 33491908 |
| Reactions occur mainly in the UVA range (315–400 nm) | 2021 review | UVA protection is central, not optional | Same review |
| Hundreds of drugs (the review compiled ~393 compounds) carry photosensitizing potential | 2021 review | Far more than the “top 5” lists imply | Same review |
| Regulators list antibiotics, NSAIDs, diuretics, retinoids and more as culprits | Current | Official, consumer-facing confirmation | FDA |
| Public medicine pages carry explicit sun warnings for tetracyclines | Current | The advice reaches patients, not just specialists | NHS, MedlinePlus |
What this means for you: the research doesn’t say “avoid these drugs.” It says the risk is real, it’s mostly the sunburn-like phototoxic type, and it’s mostly UVA-driven — a combination that’s very controllable with the right protection and, where relevant, the right prescriber conversation. Where individual risk is uncertain (skin type, dose, how much sun you actually get), it’s reasonable to admit that uncertainty and protect proactively rather than guess.
Sun-Safer Alternatives Within Each Drug Class
You can’t always avoid a photosensitizing drug — sometimes it’s simply the best treatment for you. But within several classes there are options that tend to carry lower photosensitivity risk, and it’s fair to ask your prescriber whether one fits. The table frames this as sun-safer medication alternatives, always with the same non-negotiable caveat.
| Situation | Higher-photosensitivity option | Often lower-risk option in the same situation | The catch |
|---|---|---|---|
| Common bacterial infection | Doxycycline (tetracycline) | Azithromycin, where clinically appropriate | Only the prescriber knows if the bug and your history allow the swap |
| High blood pressure | Hydrochlorothiazide (thiazide) | A different antihypertensive class | Blood-pressure control comes first — never a DIY change |
| Pain / inflammation | Piroxicam, ketoprofen gel | A shorter-acting NSAID or non-photosensitizing option | Depends on your condition and other meds |
| Acne | Certain photosensitizing agents | A regimen built around diligent sun protection | Efficacy vs sun risk is an individual trade-off |
| Non-drug baseline | (any of the above) | Physical photoprotection: clothing, timing, shade | Always available, always additive |
On antibiotics specifically, the doxycycline-versus-azithromycin question comes up constantly. We’ve compared them in depth — is azithromycin a sun-safer swap than doxycycline? — but the short version is that azithromycin is far less associated with phototoxicity, when it’s an appropriate choice for the infection, which only your clinician can judge.
The verdict: for a short antibiotic course in someone about to spend serious time outdoors, raising the sun-sensitivity question with your prescriber is genuinely worthwhile — a lower-risk option sometimes exists. For heart and blood-pressure medicines, the calculus flips: the cardiovascular protection almost always outweighs the sun nuisance, so the answer is better protection, not a switch, unless your prescriber initiates one. And for everyone, the most reliable “alternative” isn’t a different pill at all — it’s the physical protection in the next section, which lowers your risk no matter what you take.
How to Protect Yourself — Practical Guidance
Here’s where that opening hint about your sunscreen pays off. Because drug photosensitivity is mostly UVA-driven, ordinary “SPF” — which primarily measures UVB protection — isn’t the whole story. You need genuine, high-level UVA coverage. Follow these steps in order.

- Read every label and leaflet for a sun warning. Prescription and over-the-counter alike. If a symbol or line mentions sunlight, treat it as real. When unsure, ask your pharmacist to check your full list at once.
- Choose a true broad-spectrum UVA sunscreen. Look for “broad spectrum,” a high UVA rating (PA++++ or a high UVA-PF / the UVA-in-a-circle symbol), and SPF 30 or higher. Apply generously and reapply every two hours and after swimming or sweating. This is the single highest-value step for broad-spectrum UVA sunscreen protection.
- Cover up — sunscreen isn’t a force field. A wide-brimmed hat, UPF-rated clothing, and UV-blocking sunglasses physically stop light that no lotion fully catches. For strong photosensitizers, fabric beats cream.
- Time your outdoor hours. UV peaks roughly 10am–4pm. Shift walks, sport, and errands to early morning or evening during a heat wave. Shade is free protection.
- Never change a medication on your own — call your pharmacist or doctor first. If you react, or you’re worried before a sunny trip, ask about timing, dose, or a sun-safer alternative. This matters most for heart, blood-pressure, and rhythm drugs, where stopping can be dangerous.
Mistakes to Avoid
- Assuming clouds or car windows protect you. UVA passes through both. Reactions happen on overcast days and long drives.
- Relying on SPF number alone. A high SPF with weak UVA rating under-protects against exactly the wavelength that drives drug photosensitivity.
- Forgetting topical gels. Ketoprofen gel on the skin plus sun is a classic trigger — wash it off or cover it before going out.
- Stopping a drug “just for the holiday.” Skipping antibiotics risks treatment failure; skipping heart medicines risks far worse. Protect instead, and consult first.
If you want to check what you’re taking against the list, you can browse the full antibiotics range to see which agents come with sun warnings — but the label and your pharmacist remain your best sources for your specific medicines.
Related Reading
- How tretinoin and sun exposure interact — the retinoid deep-dive that pairs with this umbrella guide.
- Is azithromycin a sun-safer swap than doxycycline? — the antibiotic comparison in full.
- See heart & blood-pressure medication options — background before a prescriber conversation about alternatives.
Frequently Asked Questions
Which antibiotics make you sensitive to the sun?
Tetracyclines — especially doxycycline — are the antibiotics most strongly linked to sun sensitivity, followed by fluoroquinolones (like ciprofloxacin) and the sulfonamide combination co-trimoxazole. These cause mostly phototoxic reactions, meaning an exaggerated, sometimes blistering sunburn on exposed skin. Public sources including the NHS and MedlinePlus carry explicit sun warnings for doxycycline. If you’re on one, protect diligently and ask your pharmacist about your specific antibiotic.
How long does drug-induced sun sensitivity last?
For phototoxic reactions, sensitivity generally fades within days of stopping the drug — but only your prescriber should decide whether stopping is appropriate. Some medicines, like amiodarone, stay in the body for weeks to months, so the sensitivity lingers accordingly. Photoallergic reactions can occasionally persist longer. As a rule, plan protection for the whole time you’re on a photosensitizing drug, plus a buffer afterward.
Can blood pressure medication cause sunburn?
Yes. Thiazide diuretics such as hydrochlorothiazide are among the more common photosensitizers, and they’re widely used for blood pressure. The reaction is usually a phototoxic, sunburn-like response, sometimes more persistent than an ordinary burn. The critical point: never stop a blood-pressure medicine because of the sun. Protect your skin thoroughly, and if you react, ask your doctor whether a sun-safer alternative suits you.
What does a phototoxic reaction look like?
It looks like a severe, often rapid sunburn — redness, heat, stinging, sometimes blistering or swelling — confined to skin that saw the sun. It can appear within hours and is out of proportion to your actual exposure. That “too much burn for too little sun” mismatch is the classic clue. It differs from a photoallergic reaction, which is itchier, eczema-like, and shows up a day or more later.
Does sunscreen work against drug-induced photosensitivity?
It helps significantly, but the type matters. Because these reactions are mostly UVA-driven, you need a genuine broad-spectrum UVA sunscreen (high UVA rating plus SPF 30+), not just a high SPF number, which mainly reflects UVB protection. Even the best sunscreen works best alongside protective clothing, a hat, and avoiding peak-UV hours. For strong photosensitizers, physical cover-up is your most reliable layer.
Should I stop my medication in summer to avoid sun sensitivity?
No — not on your own. Stopping antibiotics can cause treatment failure and resistance; stopping heart, blood-pressure, or rhythm medicines can be dangerous. The right approach is to protect against the sun and, if the reaction bothers you, talk to your doctor or pharmacist about timing, dose, or a sun-safer alternative. Any change should be a professional decision, never a DIY one.
Is St John’s wort really a sun-sensitivity risk?
Yes. St John’s wort contains hypericin, a recognised photosensitizer, so a “natural” supplement can behave like a photosensitizing drug. It’s a good reminder to tell your pharmacist about every supplement, not just prescriptions — herbal products can also interact with other medicines you take.
Medical Disclaimer
This article is for general information and education only and is not a substitute for professional medical advice, diagnosis, or treatment. Do not start, stop, or change any medication based on this content. Photosensitivity risk, severity, and the suitability of any alternative depend on your individual health, other medicines, and circumstances. Always talk to your doctor or pharmacist first, and seek prompt medical care for severe skin reactions, blistering, facial swelling, or signs of overheating.
The Bottom Line
Here’s the balanced verdict. Medications that cause sun sensitivity are common, the reactions are mostly the manageable phototoxic kind, and the risk is highly controllable — you rarely have to choose between your treatment and the summer. What you do have to do is know which of your medicines are on the list, protect against UVA specifically, and loop in your prescriber before changing anything, especially heart and blood-pressure drugs.
Your one immediate action: pull out every medication and supplement you currently take and check each label and leaflet for a sun warning today — before your next sunny afternoon. If you find one, add a real broad-spectrum UVA sunscreen and cover-up to your routine, and put a question to your pharmacist on your next visit.
Wondering whether a lower-risk antibiotic fits your situation? Read is azithromycin a sun-safer swap than doxycycline next. And if you keep cycling through antibiotics for repeat urinary infections — remember that several of those UTI antibiotics (fluoroquinolones and TMP-SMX) sit right on this photosensitizer list — see our companion guide on why several UTI antibiotics are on this list, and the estrogen option that cuts repeat infections. Your next sunny day shouldn’t cost you a week of blistered skin — a five-minute cabinet check makes sure it doesn’t.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.