







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
One glass of grapefruit juice can raise the blood level of the blood-pressure drug felodipine to roughly three times what water produces — and with regular grapefruit, up to five times. That is not a rumour; it is the finding that opened modern research into grapefruit drug interactions. More than 85 medicines are now known or predicted to react with grapefruit, and around 43 of them can trigger serious problems.
So if a pharmacist told you “no grapefruit,” they were not being fussy. Grapefruit and medications are a genuinely well-documented mismatch. But here is the part most warning labels skip: the risk is not equal across every drug, the effect can last far longer than you would guess, and — surprisingly — grapefruit makes a few medicines weaker, not stronger. By the end of this guide you will know exactly which tier your medicine sits in, how much grapefruit actually matters, and what to safely ask your prescriber about instead.
One detail near the end surprises almost everyone: skipping grapefruit “just on the morning you take your pill” does not protect you. We will explain why in the mechanism section — and it changes the whole rulebook.
Key Takeaways
- 85+ medicines interact with grapefruit — but only some are dangerous; we sort them into three clear tiers.
- One small glass can count. A single serving already tripled felodipine levels in studies — you do not need a jug.
- The effect lingers up to ~3 days, so changing when you take the pill usually will not save you.
- Not all statins are equal — one is a red flag, another barely reacts. The difference is the whole game.
- A few drugs get weaker with grapefruit (yes, really) — an effect almost no list mentions.
- It is not just grapefruit — one common breakfast fruit shares the risk, and it hides in marmalade.
On this page
Grapefruit Drug Interactions: What They Really Are
Grapefruit drug interactions happen when compounds in grapefruit change how your body absorbs or clears a medicine, so you end up with too much drug in your blood — or occasionally too little. The result can be stronger side effects, a weaker medicine, or, with a handful of drugs, a genuinely dangerous overdose-level exposure from a normal dose.
That is the 40-second version. Now the useful detail.
Most food-and-drug advice is vague (“avoid certain foods”). Grapefruit is different because the science is unusually precise: it is one of the best-studied foods that interact with medications, so we know the exact chemicals responsible, the exact enzyme they hit, and roughly how long the effect lasts. That precision is good news for you, because the rules linking grapefruit and medications are learnable rather than mysterious.
Here is the key mental model. Your body treats most medicines as substances to be broken down and removed at a steady, predictable pace. That predictable pace is what your prescribed dose is built around. Anything that speeds up or slows down that pace changes the effective dose — even though the number on the tablet never changes. Grapefruit slows the pace for many drugs, so the same tablet suddenly acts like a bigger one.
The single most important idea in this whole article: grapefruit does not change your pill — it changes you, specifically the enzyme that processes the pill. Hold that thought; it explains everything that follows.
How Grapefruit Hijacks Your Gut — CYP3A4 Inhibition in Plain English
Deep in the lining of your small intestine sits an enzyme called CYP3A4. Think of it as a row of gatekeepers standing at the border between your gut and your bloodstream. When you swallow many common medicines, these gatekeepers grab a large share of the drug and break it down before it ever reaches your blood. Your dose is calculated assuming those gatekeepers are doing their usual job.
Grapefruit contains natural compounds called furanocoumarins. When they arrive, they do not simply distract the gatekeepers — they permanently disable them. Pharmacologists call this “mechanism-based,” or irreversible, inhibition: the CYP3A4 enzyme is not just blocked, it is destroyed.
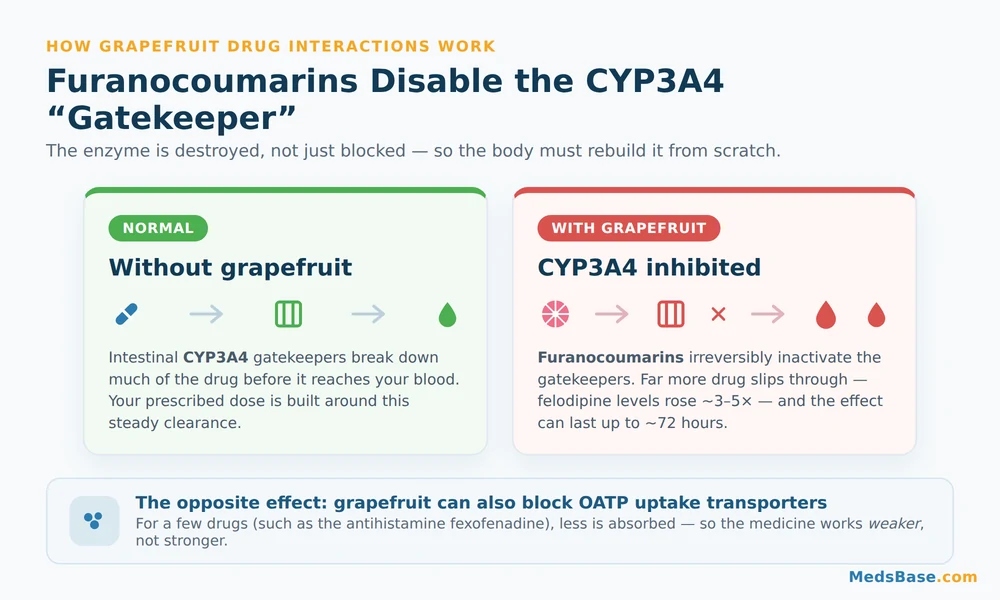
Here is where it gets interesting. Because the enzyme is destroyed rather than temporarily occupied, your body cannot just wait for the grapefruit to wash out. It has to build brand-new enzyme from scratch. According to the FDA, that recovery is slow — the effect of grapefruit can linger for up to about 72 hours (FDA consumer update).
That single fact demolishes the most common myth about any grapefruit juice drug interaction. People assume they can eat grapefruit at breakfast and take their pill at night and stay safe. They cannot — for a strongly-interacting drug. The gatekeepers you wiped out this morning are still gone tonight, and largely gone tomorrow. For serious interactions, timing does not fix the problem; only avoidance does. That is the open loop from the intro, now closed.
With fewer gatekeepers, far more of your drug slips straight into the bloodstream. For felodipine, a single ordinary serving of grapefruit juice produced an average blood level about three times that seen with water; with repeated grapefruit, roughly five times (Bailey et al., CMAJ 2013). A three-to-five-fold jump from breakfast is exactly why this matters.
Research Spotlight
The landmark 2013 CMAJ review by Bailey and colleagues catalogued more than 85 interacting drugs and identified about 43 capable of serious outcomes — including dangerously low blood pressure, muscle breakdown (rhabdomyolysis), and kidney injury. It also confirmed the mechanism: furanocoumarins irreversibly inactivate intestinal CYP3A4, and normal function returns only as the body synthesises fresh enzyme.
The plot twist: grapefruit can make some drugs weaker
Almost every “grapefruit list” online stops at “drugs get stronger.” That is only half the biology. Grapefruit also blocks a second system — uptake transporters called OATP — which some drugs rely on to get into your blood in the first place. Block those, and less drug is absorbed.
The classic example is fexofenadine, a common non-drowsy antihistamine, and it is the grapefruit juice drug interaction that runs backwards. In studies, grapefruit juice cut fexofenadine absorption substantially — roughly to half or less of the level seen with water, depending on how much juice was taken. So for a handful of medicines, grapefruit does not overdose you; it quietly under-doses you, and your allergy tablet or thyroid-adjacent drug simply works less well. This is why “grapefruit interacts with medications” is more nuanced than a scare headline — direction matters, and it is drug-specific.
Bottom line on mechanism: grapefruit strongly slows the clearance of many CYP3A4 drugs (stronger, sometimes dangerously) and reduces the uptake of a few OATP drugs (weaker). Both are real; both are why blanket rules fail.
Which Medications Interact — The Severity Tiers
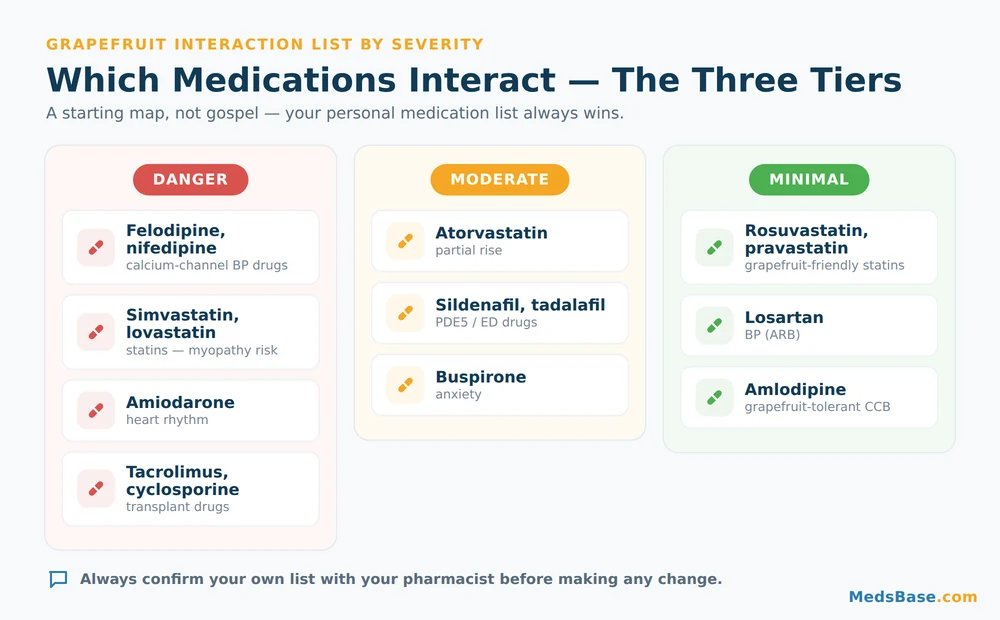
This is the section you came for. Below is a grapefruit interaction list sorted by how much it actually matters — not just an alphabetical dump. Treat this grapefruit interaction list as a starting map, then confirm your own drugs against it. Read it as guidance, not gospel: your personal medicines, doses, and health history always override any chart, which is why every swap column ends in “ask your prescriber.”
| Drug / class | What grapefruit does | Severity | Safer alternative to ask about |
|---|---|---|---|
| Felodipine, nifedipine (calcium-channel BP drugs) | Blood levels can rise 3–5×; risk of blood-pressure crash, dizziness, flushing | Danger | Amlodipine interacts minimally — ask your prescriber |
| Simvastatin, lovastatin (statins) | AUC up to ~330–700%; raises muscle-damage (myopathy) risk | Danger | Rosuvastatin or pravastatin barely interact — ask your prescriber |
| Amiodarone (heart rhythm) | Higher levels; risk of rhythm and QT effects | Danger | Individualised — never adjust yourself; specialist only |
| Tacrolimus, cyclosporine (transplant immunosuppressants) | Unpredictable spikes; toxicity/kidney risk | Danger | No casual swap — strict avoidance, specialist-managed |
| Some older antihistamines (historically terfenadine, astemizole — largely withdrawn) | Dangerous heart-rhythm effects (why they were pulled) | Danger (historical) | Modern antihistamines are the safer standard |
| Atorvastatin (statin) | Partial rise (AUC ~180–250%); real but smaller than simvastatin | Moderate | Rosuvastatin if grapefruit is a fixture in your diet — ask your prescriber |
| Sildenafil, tadalafil (PDE5 / ED drugs) | Mild-to-moderate rise in blood level; usually a nuisance, not a crisis | Moderate | Discuss timing/interactions with your prescriber, especially with nitrates |
| Buspirone (anxiety) | Levels can climb several-fold; more drowsiness/dizziness | Moderate | Ask about dose or an alternative if you eat grapefruit often |
| Rosuvastatin, pravastatin (statins) | Little to no interaction (not mainly CYP3A4-cleared) | Minimal | Often the grapefruit-friendly statin choice — confirm with prescriber |
| Losartan (BP, ARB) | Minimal / clinically minor | Minimal | Generally fine — confirm your specific regimen |
| Amlodipine (BP, calcium-channel) | Minimal, unlike felodipine/nifedipine | Minimal | The grapefruit-tolerant CCB — confirm with prescriber |
Figures for felodipine, simvastatin, lovastatin and atorvastatin are drawn from Bailey et al., CMAJ 2013. Sildenafil, tadalafil and buspirone effects are described in general terms here — the exact fold-increase varies by study and person; confirm specifics with your pharmacist.
Notice the pattern that runs through the whole table: within the same drug class, one member can be a red flag and another almost inert. Nowhere is this clearer than with statins and grapefruit. Simvastatin sits in the danger tier; rosuvastatin sits in the green. If you love grapefruit and take a statin, that difference is not trivia — it is potentially the single most useful thing on this page. It is also exactly the kind of nuance we compare in depth in our guide to how the two most-prescribed statins actually differ, because the grapefruit angle is only one of several ways they diverge.
Who this matters most for — and who can relax
Pay close attention if you take: a calcium-channel blood-pressure drug (felodipine/nifedipine), simvastatin or lovastatin, amiodarone, or a transplant immunosuppressant. You can usually relax if you take: rosuvastatin, pravastatin, losartan, or amlodipine — though “usually” is not “always,” so still confirm your personal list. Never assume a whole class is safe or unsafe based on one drug — that error is how people get caught.
If you are reviewing a blood-pressure or heart medicine against this list, our blood-pressure and heart medicines category groups the common options so you can see which one you are actually on before you raise it with your prescriber. And if you are on a statin, MedsBase carries several including grapefruit-tolerant options like rosuvastatin — a good prompt to compare, not switch on your own.
A quick, soft note for the ED-medicine crowd: sildenafil and tadalafil land in the moderate tier, so an occasional grapefruit is rarely a drama. If that is your situation, the ED medicines and how they’re taken category explains the usual dosing — but always flag any grapefruit habit to your prescriber, particularly if you also take nitrates or alpha-blockers.
Side Effects, How Much Matters, and What To Do
So what does a grapefruit interaction actually feel like? It depends entirely on the drug — because grapefruit does not create new side effects, it amplifies the ones the drug already carries. Here is how the most common scenarios show up and what to do.
| What you might notice | With which drugs | Severity signal | What to do |
|---|---|---|---|
| Dizziness, light-headedness, flushing | Felodipine, nifedipine, other BP drugs | Can be serious if BP drops sharply | Sit/lie down; contact your prescriber; do not “push through” repeated episodes |
| Muscle aches, weakness, dark urine | Simvastatin, lovastatin (myopathy signal) | Red flag — possible muscle breakdown | Stop grapefruit, seek medical advice promptly — do not stop the statin on your own |
| Extra drowsiness, unsteadiness | Buspirone, some sedating drugs | Usually moderate | Review with pharmacist; avoid driving until clear |
| Allergy tablet “stopped working” | Fexofenadine (OATP effect) | Mild but frustrating | Separate the juice from the dose or skip grapefruit; ask pharmacist |
| Palpitations, faint feeling | Amiodarone, historical antihistamines | Potentially serious (rhythm) | Urgent medical advice; specialist-managed drugs — strict avoidance |
How much grapefruit is “too much”? Less than you think. This is where the myths cluster, so let us clear them one by one:
- “A small glass is fine.” Not for strong interactions. A single ordinary serving already tripled felodipine levels in research. Volume increases the effect, but even one glass is enough to matter for danger-tier drugs.
- “Juice is the problem, not the fruit.” Both count. Whole grapefruit and the juice contain the same furanocoumarins. Segments in a fruit salad are not a loophole.
- “I’ll just take my pill at a different time of day.” For strong interactions, no. Because the enzyme is destroyed and takes days to rebuild, separating the pill and the grapefruit by a few hours does not reliably protect you. This is the myth we flagged at the very start — now you know why it fails.
- “One grapefruit years ago never hurt me, so it’s fine.” Individual biology varies. The amount of CYP3A4 you have differs from the next person’s, so the same grapefruit and the same drug can affect two people quite differently, as the FDA notes. “It was fine before” is not a safety guarantee.
The honest, non-alarmist summary: for green-tier drugs, grapefruit is a non-issue and you can enjoy it. For red-tier drugs, treat grapefruit and its cousins as off the menu entirely while you are on the medicine — not a timing puzzle to solve. When you are unsure which tier you are in, that uncertainty is itself the signal to ask a pharmacist. Pharmacists commonly see patients who carefully changed their dosing time to “work around” grapefruit, not realising that for their particular statin, only avoidance would have helped.
What the Research Actually Shows
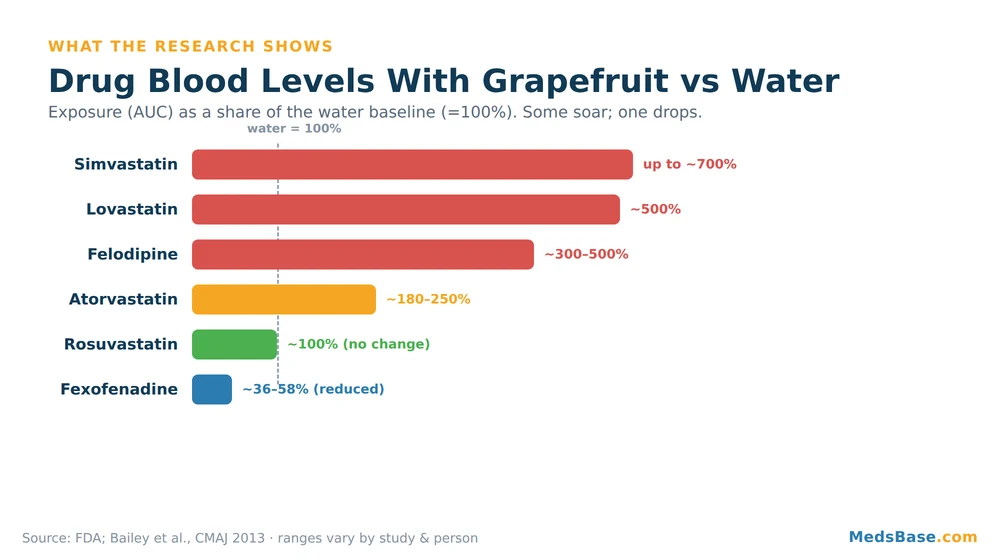
The evidence base here is unusually solid for a food-drug topic, because these interactions have been measured directly in controlled studies. Here is a snapshot, with qualifying language where the science is still individual.
| Finding | Year | What it showed | Source |
|---|---|---|---|
| >85 drugs interact; ~43 can cause serious effects | 2013 | Comprehensive catalogue + confirmed irreversible CYP3A4 mechanism | CMAJ (Bailey et al.) |
| Felodipine ~3× (single serving) up to ~5× (repeated) | 2013 | One glass is enough to matter; more grapefruit, larger effect | CMAJ |
| Simvastatin AUC ~330% (usual) up to ~700% (high volume); lovastatin ~500% | 2013 | Statins vary enormously — some soar, some barely move | CMAJ |
| Effect can persist up to ~72 hours | current | Timing tricks do not defeat a strong interaction | FDA |
| Grapefruit can reduce fexofenadine absorption (OATP) | 2013+ | A few drugs get weaker, not stronger | CMAJ |
What this means for you: the numbers confirm the practical rules rather than replacing them. You do not need to memorise a percentage — you need to know your drug’s tier and, when it is red, avoid grapefruit fully. Where evidence is genuinely individual (how much your enzyme level shifts, how much you are affected), the honest answer is “it varies, so err on the side of caution and ask.” Admitting that variability is not a weakness in the advice; it is the whole reason a personalised pharmacist check beats any generic list.
Grapefruit vs the Other Citrus — The Cousin Nobody Warns You About
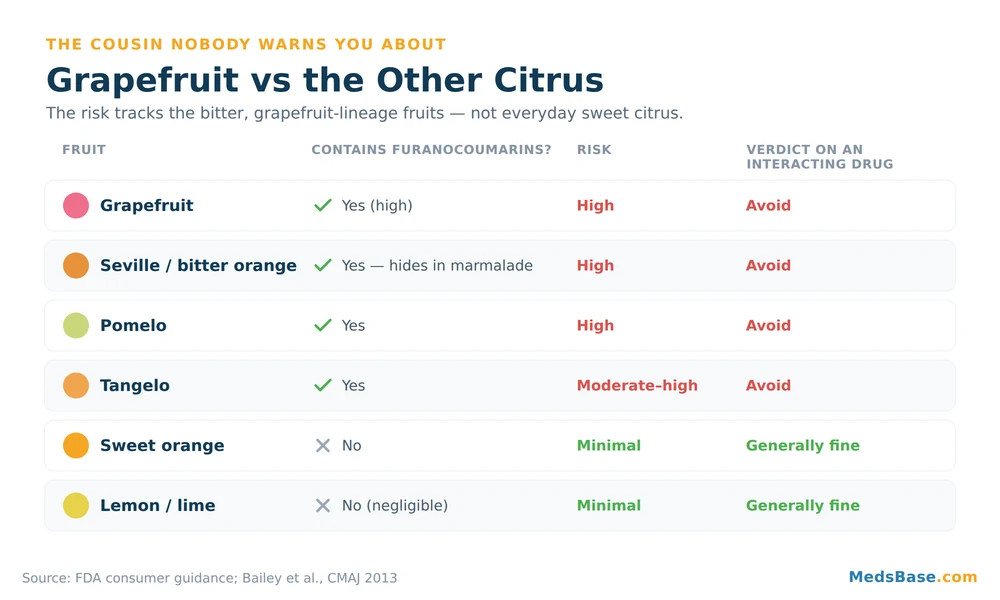
Here is a trap that catches careful people: they dutifully avoid grapefruit, then get an interaction anyway — from marmalade. That is because furanocoumarins are not unique to grapefruit. Several citrus relatives share them, while everyday oranges and lemons do not. If your drug interacts with grapefruit, it interacts with the whole furanocoumarin family.
| Citrus | Contains furanocoumarins? | Interaction risk | Verdict if you’re on an interacting drug |
|---|---|---|---|
| Grapefruit | Yes (high) | High | Avoid |
| Seville / bitter orange (marmalade!) | Yes | High | Avoid — including marmalade |
| Pomelo | Yes | High | Avoid |
| Tangelo (tangerine × grapefruit) | Yes | Moderate–high | Avoid |
| Sweet orange (the usual breakfast orange) | No | Minimal | Generally fine |
| Lemon / lime | No (negligible) | Minimal | Generally fine |
The verdict: the risk tracks the bitter, grapefruit-lineage fruits — grapefruit, Seville oranges, pomelos and tangelos — not the sweet everyday citrus. Your normal glass of orange juice and your lemon-in-water are not the problem, per the FDA’s guidance. But “orange marmalade” is frequently made from Seville oranges, which is exactly why this cousin catches people off guard.
Think of it like the statin story we mentioned earlier: within one family, some members are risky and some are safe, and the label alone won’t tell you which. That “same family, opposite risk” logic is the single most useful pattern to carry with you — and it is precisely why we mapped it out in detail for statins in our statin comparison guide.
Your Five-Minute Safety Routine + Pharmacist Script
You do not need to become a pharmacologist. You need a repeatable routine. Here is the exact one, formatted so you can follow it in order.
- List everything you take — prescription drugs, over-the-counter medicines, and supplements. Grapefruit does not care whether a bottle needs a prescription.
- Read each label and leaflet for the word “grapefruit.” Manufacturers are required to flag known interactions; MedlinePlus is a reliable plain-language backup for checking any drug (MedlinePlus).
- Call your pharmacist with the short script below. This is the step most people skip — and it is the one that actually protects you.
- If any drug interacts, avoid grapefruit and its cousins entirely while you take it. Do not try to “time around” a strong interaction.
Your 20-second pharmacist call script:
“Hi — I take [drug names]. I’d like to know: does grapefruit interact with any of them, is it a serious interaction or a minor one, and if it’s serious, is there a grapefruit-friendly alternative in the same class I could ask my doctor about?”
That last clause is the gold. It moves you from “just avoid grapefruit forever” to “maybe there’s a better-fitting drug for my life” — a conversation only your prescriber can conclude, but one you are now equipped to start.
Common mistakes to avoid:
- Assuming “natural” grapefruit is automatically gentle — the interaction is chemical, not about being natural.
- Checking only prescriptions and ignoring supplements or OTC medicines.
- Changing your dose yourself instead of changing your grapefruit — never adjust medication on your own.
- Forgetting marmalade, pomelo, and “citrus blend” juices.
- Assuming a green-tier drug today stays green if your prescription changes — re-check after any new medicine.
The NHS makes the same practical point for statins specifically: for the strongly-interacting ones, the guidance is to avoid grapefruit, not to fine-tune the clock (NHS).
Related reading
- Other everyday medicines with a hidden catch — grapefruit isn’t the only quiet risk on your shelf.
- How the two most-prescribed statins compare — the grapefruit split explained in full.
- Supplements can interact too — why “it’s just a supplement” is a myth worth retiring.
Frequently Asked Questions
How long does grapefruit affect medications?
Up to about 3 days. Because grapefruit’s furanocoumarins irreversibly destroy the CYP3A4 enzyme, your body has to build new enzyme before things return to normal — a process that can take up to roughly 72 hours according to the FDA. That is why separating your pill from grapefruit by a few hours does not reliably protect you against a strong interaction; the enzyme is still depleted the next day.
Can I eat grapefruit with statins?
With statins and grapefruit, it depends on the statin. Simvastatin and lovastatin can rise dramatically with grapefruit and belong in the “avoid” group. Atorvastatin has a smaller but real interaction. Rosuvastatin and pravastatin barely interact and are often the grapefruit-friendly choice. Never switch statins on your own — ask your prescriber which one fits your diet and health profile.
Is one grapefruit enough to cause an interaction?
Yes, for strongly-interacting drugs. In research, a single ordinary serving of grapefruit juice was enough to roughly triple felodipine blood levels. More grapefruit increases the effect, but you do not need large amounts — one glass or one whole fruit can matter for danger-tier medicines.
Which blood pressure medications interact with grapefruit?
When it comes to grapefruit and blood pressure medication, the calcium-channel blockers felodipine and nifedipine are the notable ones — grapefruit can raise their levels several-fold and drop your blood pressure too far. Reassuringly, amlodipine (also a calcium-channel blocker) and losartan (an ARB) interact minimally. The safest habit around grapefruit and blood pressure medication is to check your specific tablet name against the tier table above and confirm with your pharmacist.
Does grapefruit interact with all statins?
No — and this is the most useful thing to know. The interaction is strong for simvastatin and lovastatin, partial for atorvastatin, and minimal for rosuvastatin and pravastatin. The difference comes down to how each statin is processed by the body. If you eat grapefruit regularly, it is worth asking your prescriber whether a low-interaction statin suits you.
What fruits are like grapefruit for drug interactions?
Seville (bitter) oranges — the kind used in marmalade — plus pomelos and tangelos share grapefruit’s furanocoumarins and carry similar risk. Ordinary sweet oranges, lemons, and limes do not, so your usual orange juice is generally fine. If a drug interacts with grapefruit, treat the whole bitter-citrus family as off-limits.
Do grapefruit interactions affect ED medicines like sildenafil?
There is a mild-to-moderate effect. Grapefruit can modestly raise sildenafil and tadalafil blood levels, which is usually a nuisance rather than a danger. Still mention any grapefruit habit to your prescriber, especially if you also take nitrates or alpha-blockers, where any exaggeration of blood-pressure effects deserves attention.
Can grapefruit ever make a medicine weaker?
Yes — a detail most guides miss. Grapefruit blocks OATP uptake transporters that some drugs (such as the antihistamine fexofenadine) need to be absorbed. For those medicines, grapefruit reduces the amount reaching your blood, so the drug works less well. It is another reason to check your specific medicine rather than assume grapefruit always makes things “stronger.”
The Bottom Line on Grapefruit Drug Interactions
Grapefruit drug interactions are real, sometimes serious, but entirely manageable once you know your tier. The evidence is clear: more than 85 medicines interact, roughly 43 can cause serious harm, the effect can persist for about three days, and for a few drugs grapefruit actually works in reverse. The single biggest mistake is treating it as a timing problem — for strong interactions, only full avoidance of grapefruit and its bitter-citrus cousins works.
Grapefruit is simply one of the best-known foods that interact with medications — and one of the most avoidable, once you know your tier. Your one immediate action: take five minutes today to list your medicines and supplements, then read each label for the word “grapefruit” — and if you see it, or you are unsure, call your pharmacist with the script above before your next glass. Do not stop or switch any medication on your own; the goal is an informed conversation, not a solo decision.
The reassuring flip side: if you take a green-tier drug, grapefruit is genuinely fine, and you can stop worrying. Most of the anxiety around this topic comes from not knowing which tier you are in — and now you do.
Still curious how everyday drugs carry risks you never signed up for? Two natural next reads: our guide to other everyday medicines with a hidden catch, and — for the same “the effect nobody warned you about” theme in a very different corner of medicine — another effect people never see coming with today’s most talked-about weight-loss drugs.
Medical Disclaimer
This article is for general educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Medication interactions vary between individuals. Never start, stop, switch, or adjust any medicine — or change your diet around a medicine — without first consulting your doctor or pharmacist, who can review your full medication list and health history.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.