







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
The names sound almost identical — swap one letter and you go from a four-to-six-month course that can cure severe acne for years to a nightly cream people use for wrinkles. That’s the gap between isotretinoin and tretinoin, and it’s why mixing them up is one of the most common mistakes people make when researching acne treatment online.
Both are retinoids. Both are vitamin-A derivatives. Both unclog pores and normalise skin-cell turnover. But they are fundamentally different drugs with different routes of delivery, different side-effect profiles, and different patient populations. This guide covers the real-world isotretinoin vs tretinoin comparison — how each one works, what the clinical data shows, who each treatment is actually for, and how to use them safely.
Key Takeaways
- Isotretinoin is oral (capsules, e.g. Accutane, Roaccutane, Isotroin). Tretinoin is topical (cream or gel, e.g. Retin-A, Retino-A).
- Isotretinoin is the most effective acne treatment in medicine — around 85% clearance after a full course, with many patients staying clear for years.
- Tretinoin is the gold-standard topical retinoid for mild-to-moderate acne, photoaging, hyperpigmentation and skin texture.
- Isotretinoin is absolutely contraindicated in pregnancy due to severe birth defects; tretinoin is category C and also avoided in pregnancy.
- Isotretinoin needs blood monitoring and pregnancy testing; tretinoin only needs visual follow-up.
- They are not interchangeable. The choice depends on acne severity, prior treatment response, and whether systemic therapy is warranted.
Jump to a section
What Are Isotretinoin and Tretinoin?
Quick Answer: What’s the difference?
Isotretinoin is an oral capsule reserved for severe, scarring, or treatment-resistant acne — it reduces oil production body-wide for 4 to 6 months. Tretinoin is a topical cream or gel used long-term for mild-to-moderate acne and anti-aging, working only where it is applied on the skin surface.
Isotretinoin and tretinoin are both retinoids — a class of compounds derived from, or chemically related to, vitamin A. Retinoids have been used in dermatology for more than forty years because they regulate skin-cell growth, reduce inflammation, and normalise oil-gland activity. But the similarity largely ends at their chemistry.
Isotretinoin (13-cis-retinoic acid) is a systemic medication taken by mouth as a soft gelatin capsule, typically at 10 mg to 40 mg daily. It was first approved by the US FDA in 1982 under the brand name Accutane (Roche), later marketed internationally as Roaccutane, Oratane, and sold generically today as Isotroin, Isofair, Isopil, Tretiva, Tretizen, Accufine, Tufacne and others. It is reserved for severe nodulocystic acne, scarring acne, or moderate acne that has not responded to lesser treatments.
Tretinoin (all-trans-retinoic acid, or ATRA) is a topical formulation applied directly to the skin as a cream, gel, or microsphere gel, usually in concentrations of 0.025%, 0.05%, or 0.1%. First approved in 1971 under the brand name Retin-A, it remains one of the most prescribed topical medications in dermatology — sold globally as Retin-A, Retino-A, A-Ret, Tretinex, Tretiheal, and dozens of generics.
One helpful way to remember the difference: both are retinoic acids, but isotretinoin is the one you swallow and tretinoin is the one you apply. They share a molecular skeleton but act on the body in radically different ways because of how and where they enter the skin.
How Do Isotretinoin and Tretinoin Work?
Acne forms when four things go wrong at once: oil glands produce too much sebum, dead skin cells fail to shed properly, a skin bacterium (Cutibacterium acnes) overgrows in the clogged pore, and inflammation follows. Both retinoids interrupt these processes — but they reach the follicle from opposite directions.
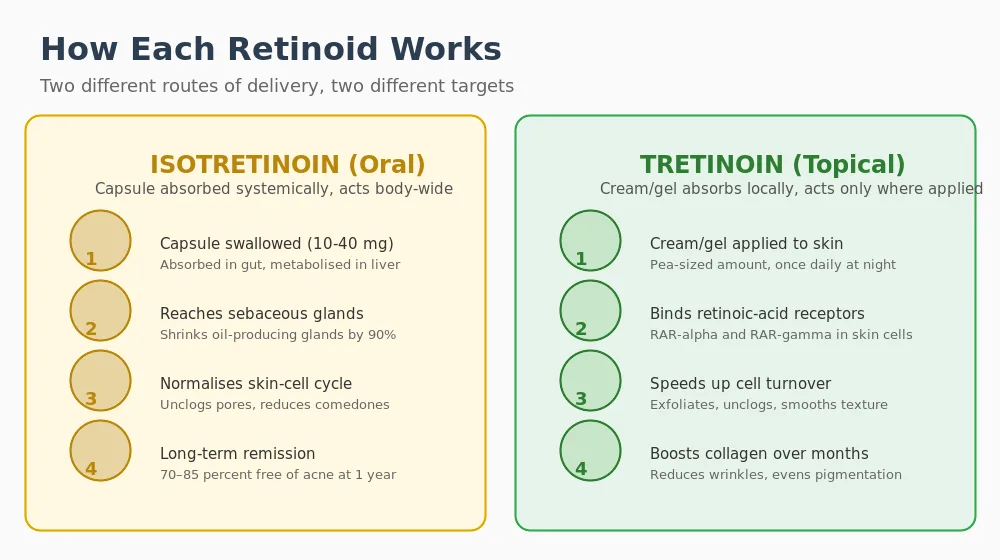
Isotretinoin: the only drug that shrinks oil glands
Swallowed isotretinoin is absorbed through the gut, taken up by the liver, then distributed in the bloodstream to tissues all over the body — including the sebaceous (oil) glands in the skin. Once inside sebocytes, it triggers apoptosis (programmed cell death) of oil-producing cells and reduces sebaceous gland size by up to 90% over a typical course.
That single property is unique. No other acne drug, topical or oral, durably shrinks oil glands. Reduce sebum output by 90% and the fuel source for acne is effectively gone — which is why around 70-85% of patients remain acne-free for years after finishing a course, even without any maintenance therapy.
Isotretinoin also normalises keratinisation in the follicle (so dead skin cells shed properly), reduces C. acnes numbers indirectly by drying up the oily environment it thrives in, and has direct anti-inflammatory effects on the skin.
Tretinoin: a receptor-level signal to turn over skin
When you rub tretinoin cream onto your face, it crosses the stratum corneum into living skin cells, where it binds to nuclear receptors called RAR-alpha, RAR-beta, and RAR-gamma. These receptors sit on DNA and control which skin-cell genes get expressed.
The result: keratinocytes (skin-surface cells) mature and shed faster, so dead cells don’t pile up and block pores; micro-comedones (the precursor lesion of every acne breakout) break up; collagen production in the dermis increases over months; and pigmentation evens out. What tretinoin does not do is shrink oil glands or enter the bloodstream in any meaningful amount — less than 2% of a topical dose is absorbed systemically in normal use.
In short: isotretinoin works from the inside out, reducing oil production body-wide, while tretinoin works from the outside in, speeding up the skin’s natural renewal where it is applied. The mechanisms are complementary rather than overlapping, which is why some dermatologists combine topical tretinoin with oral isotretinoin in rare cases (more on that below).
Key Uses and Who Each Retinoid Is For
When isotretinoin is prescribed
Because isotretinoin carries significant risks and needs monthly monitoring, it is never a first-line therapy. Dermatologists reach for it when:
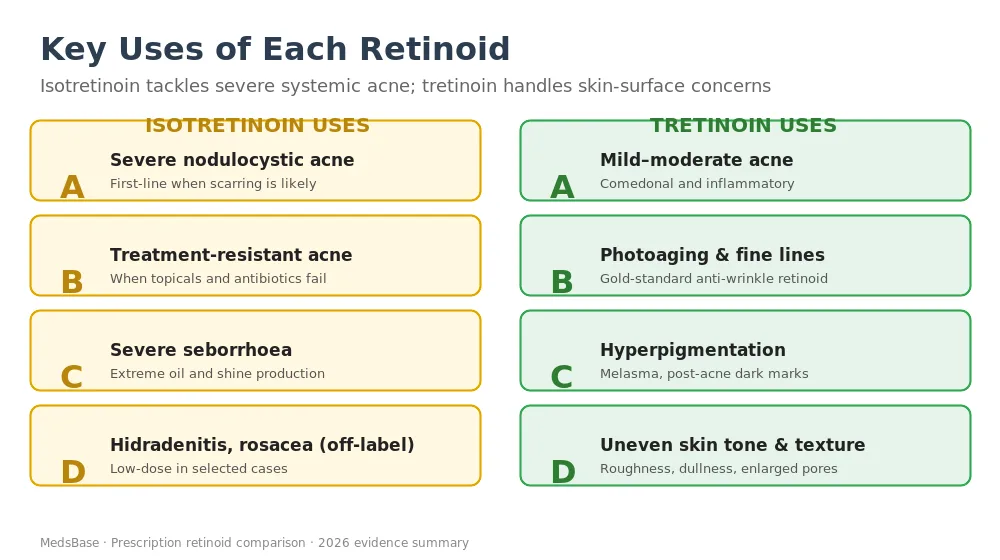
- Severe nodulocystic acne is present — large, deep, painful lesions likely to cause permanent scarring.
- Moderate acne has failed six or more months of combined topical and oral antibiotic therapy.
- Psychological distress from acne is disproportionate to its visible severity.
- Scarring is already occurring, even in moderate cases, because preventing new scars is urgent.
- Severe seborrhoea (extreme facial oiliness) accompanies acne.
When tretinoin is prescribed
Tretinoin’s indications are broader and more accessible because the side-effect profile is local and manageable. Typical uses include:
- Mild-to-moderate acne — both comedonal (blackheads, whiteheads) and inflammatory lesions.
- Photoaging — fine lines, wrinkles, and sun damage. It remains the only topical retinoid with FDA approval for photoaging.
- Hyperpigmentation — melasma, post-inflammatory hyperpigmentation (PIH) after acne, and general dullness.
- Skin texture and tone — roughness, enlarged pores, uneven colour.
- Maintenance after isotretinoin — used long-term to prevent relapse once a course is complete.
Overlap: where both can be considered
There is a narrow band of patients — moderate acne, strong psychosocial impact, partial tretinoin response — where a clinician may weigh either option. In those cases, practical factors usually decide: pregnancy plans, cost, appetite for side effects, and whether the patient has months of topical therapy already behind them.
Safety Profile, Side Effects and Dosage
Isotretinoin — expected and uncommon effects
Nearly every patient on isotretinoin experiences some mucocutaneous dryness. Most other effects are predictable, dose-related, and reversible when the drug is stopped.
| Side effect | Frequency | Severity |
|---|---|---|
| Dry lips (cheilitis) | 90%+ of users | Mild, universal — use lip balm |
| Dry skin, nose, eyes | 70-80% | Mild, manageable |
| Initial acne flare | 20-30% in first 4-6 weeks | Mild-to-moderate, temporary |
| Muscle & joint aches | 15-25% | Mild, dose-related |
| Raised triglycerides | 25-40% | Usually mild; monitored monthly |
| Raised liver enzymes | 10-15% | Usually mild and reversible |
| Mood changes / depression | Debated, <5% in trials | Variable — monitored closely |
| Teratogenicity | High if exposed in utero | Absolute contraindication in pregnancy |
Pooled from Accutane/Roaccutane product information and systematic reviews — figures vary by dose and course length.
Pregnancy prevention is non-negotiable. In countries with iPLEDGE (United States), Pregnancy Prevention Programme (UK / EU), or equivalent frameworks, women of reproductive potential must use two forms of contraception for the entire course and one month before and after.
Tretinoin — expected and uncommon effects
Tretinoin’s side effects are predictable, local, and almost always manageable with proper routine.
| Side effect | Frequency | Severity |
|---|---|---|
| Redness, peeling, dryness (“retinoid dermatitis”) | 70-90% first 4-8 weeks | Mild-to-moderate, resolves with tolerance |
| Acne purge / initial worsening | 30-50% weeks 2-8 | Temporary, part of the mechanism |
| Sun sensitivity | Universal | Significant — daily SPF essential |
| Stinging or burning on application | 30-40% | Mild, usually fades |
| Hyperpigmentation (irritation-induced) | More common in darker skin tones | Preventable with slow titration |
| Systemic absorption / teratogenicity | Very low but present | Avoid in pregnancy (Category C) |
Compiled from Retin-A prescribing information, Johnson & Johnson labelling, and clinical dermatology reviews.
Because systemic absorption is low, tretinoin does not require blood tests or monthly follow-ups. Visual clinical review every 2-3 months is sufficient.
What Does the Research Say?
The evidence base on both drugs is now decades deep. Here are the trials and reviews that most shape current guideline recommendations.
| Study | Year | Focus | Key finding |
|---|---|---|---|
| Peck et al. (NEJM) | 1979 | Isotretinoin in cystic acne | 100% clearance; most remained clear at 20-month follow-up |
| Layton (JAAD review) | 2009 | 25-year isotretinoin experience | Confirmed durability of remission and favourable risk-benefit at appropriate cumulative doses |
| Kligman et al. | 1986 | Tretinoin for photoaging | First evidence that topical tretinoin reverses sun-damage histology |
| Weinstein et al. | 1991 | Tretinoin 0.025% vs 0.1% for acne | Similar efficacy; lower strength equally effective with less irritation |
| Thiboutot et al. (AAD Guidelines) | 2018 | Acne management guideline | Isotretinoin first-line for severe/scarring acne; topical retinoids first-line for mild-to-moderate acne |
| Costa et al. (Cochrane) | 2018 | Systematic review of oral isotretinoin | Robust evidence for clearance; no convincing signal for depression risk above baseline |
| Mukherjee et al. (Clin Interv Aging) | 2006 | Tretinoin for aging skin | Review confirming measurable reductions in fine wrinkles and pigmentation over 6-12 months |
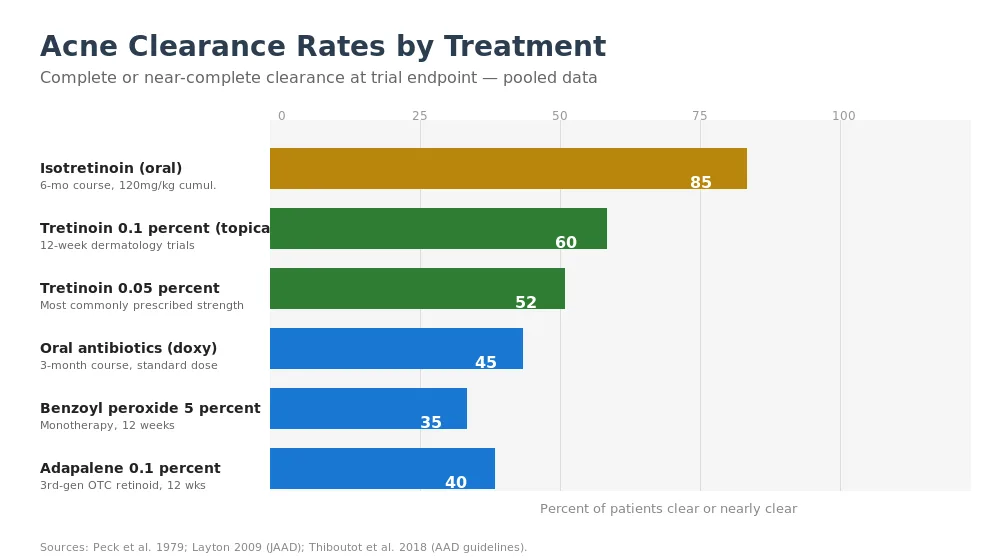
Research suggests the effect sizes are as distinct as the drugs themselves. In well-designed trials, isotretinoin achieves complete or near-complete acne clearance in roughly 85% of severe acne patients and keeps most of them clear for 2+ years after stopping. Tretinoin alone, in mild-to-moderate acne trials, typically produces a 40-60% reduction in lesion count over 12 weeks — meaningful, but not comparable to a full isotretinoin course.
Early studies indicate that tretinoin’s anti-aging effects build slowly but measurably: visible reductions in fine lines and hyperpigmentation appear between 3 and 6 months, and continue to improve over 12+ months with consistent nightly use.
Isotretinoin vs Tretinoin — Side-by-Side Comparison
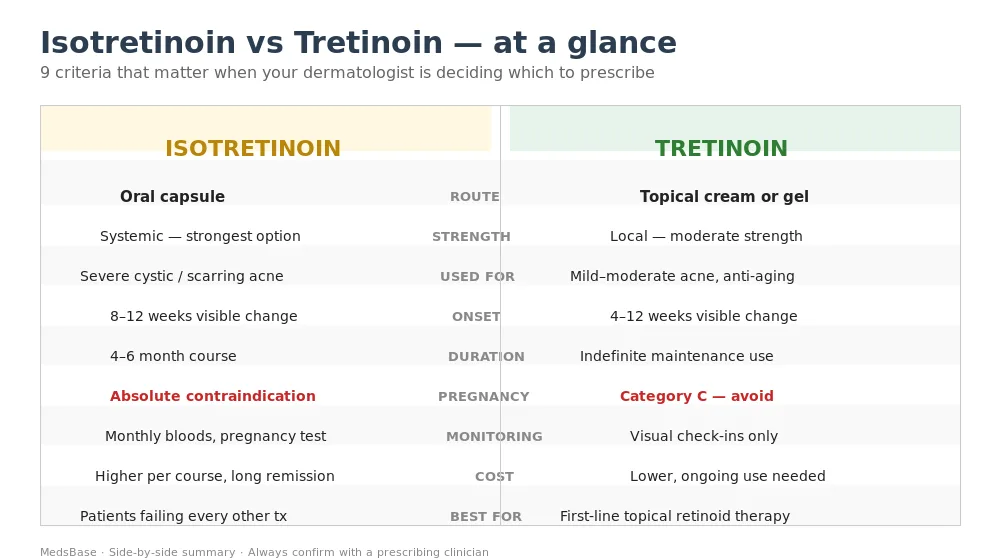
| Criterion | Isotretinoin (oral) | Tretinoin (topical) |
|---|---|---|
| Route | Oral capsule, once or twice daily | Cream or gel, nightly on clean dry skin |
| Typical strength | 10, 20, 30, 40 mg capsules | 0.025, 0.05, 0.1% cream / gel |
| Indication | Severe nodulocystic / scarring / resistant acne | Mild-to-moderate acne, photoaging, hyperpigmentation |
| Expected clearance | ~85% complete; durable remission years later | 40-60% lesion reduction at 12 weeks; ongoing maintenance |
| Course length | 4-6 months (120-150 mg/kg cumulative) | Indefinite — maintenance therapy |
| Onset of visible results | 8-12 weeks; often worsens first | 4-12 weeks; purging common |
| Monitoring | Monthly bloods + pregnancy testing | Visual review every 2-3 months |
| Pregnancy | Category X — absolute contraindication | Category C — avoid |
| Sun sensitivity | Moderate — SPF recommended | High — daily SPF 50 essential |
| Cost per month | Higher per course, but fixed endpoint | Lower, but ongoing indefinitely |
| Common brands | Accutane, Roaccutane, Isotroin, Isofair, Accufine, Tretiva | Retin-A, Retino-A, Tretinex, Tretiheal, A-Ret |
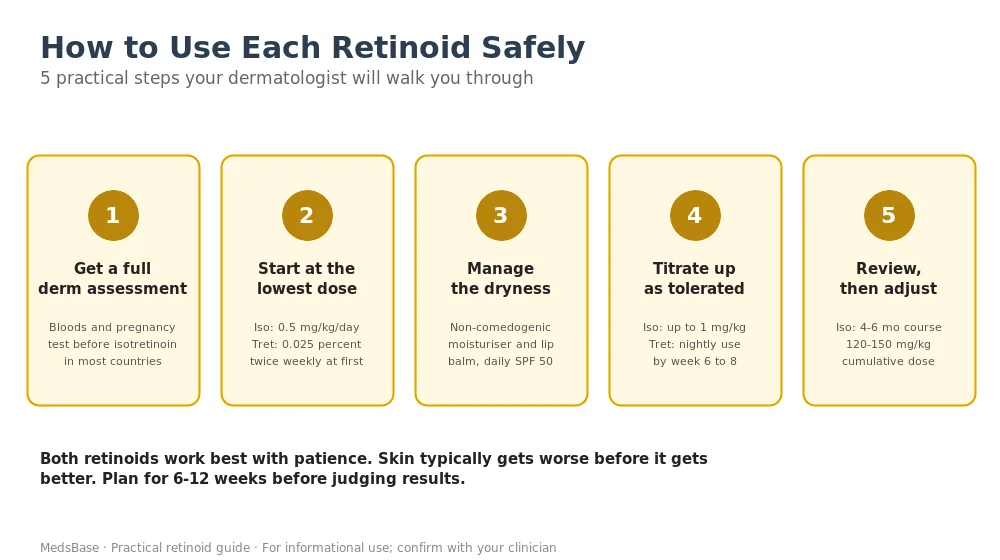
How to Use Each Retinoid — Practical Guidance
Starting isotretinoin
A full isotretinoin course follows a predictable arc. Most dermatologists start at 0.5 mg/kg/day and titrate up to 1 mg/kg/day after the first month if tolerated. The goal is a cumulative dose of 120 to 150 mg per kg body weight over 4 to 6 months.
Standard monitoring includes baseline and monthly complete blood count, liver function tests, fasting lipids, and — for women who can conceive — monthly pregnancy tests with mandatory contraception. Take capsules with a fatty meal; absorption roughly doubles when taken with food.
Expect a purge flare in weeks 2 to 6 (more common at higher starting doses), worsening dryness until month two, and steady improvement from month three onwards. Browse our full acne treatment catalogue at MedsBase including Isotroin, Isofair, Accufine, and Tretiva in multiple strengths.
Starting tretinoin
Tretinoin’s success depends almost entirely on getting the onboarding right. Most patients who “can’t tolerate” tretinoin simply started too hard and too fast. A safer protocol:
- Week 1-2: Apply a pea-sized amount of 0.025% cream twice weekly, to dry skin, at night, 20 minutes after cleansing.
- Week 3-4: Increase to every other night if tolerated.
- Week 5-8: Move to nightly if redness and peeling are under control.
- Month 3-6: Consider titrating to 0.05% or 0.1% if the lower strength has plateaued and tolerance is good.
- Always: moisturise generously each night, and use SPF 50 every morning without exception.
Shop the full tretinoin cream range at MedsBase or compare tretinoin cream versus gel formulations to pick the right vehicle for your skin. For those new to retinoids, our tretinoin versus retinol guide explains the OTC alternative in more detail.
Common Mistakes and How to Avoid Them
Most of the reasons people fail on either retinoid come down to a handful of avoidable errors. Knowing them ahead of time saves months of frustration.
Mistakes on isotretinoin
- Stopping too early. Patients often feel “cured” by month three and want to quit. Finishing the cumulative dose (120-150 mg/kg) is what delivers durable remission; cutting short raises the relapse rate substantially.
- Skipping the fatty meal. Isotretinoin absorption roughly doubles when taken with a meal containing fat. Taking it on an empty stomach can cut the effective dose in half.
- Underestimating the dryness. Dry lips, nose bleeds, and dry eyes are nearly universal. A heavy lip balm, nasal saline spray, and preservative-free artificial tears should be bought before starting, not after symptoms appear.
- Alcohol and vitamin A supplements. Both add load to the liver and can compound isotretinoin’s effects. Keep alcohol minimal and stop any separate vitamin-A supplementation for the duration of the course.
- Waxing, laser, and aggressive procedures. Skin is thin and fragile for months on isotretinoin — avoid these procedures during the course and for six months afterwards to reduce scarring risk.
Mistakes on tretinoin
- Starting too strong. Jumping straight to 0.1% nightly is the single biggest cause of tretinoin “failure” — the skin becomes so inflamed that patients quit within two weeks. Always titrate up.
- Quitting during the purge. Weeks 2 to 8 can look worse, not better. That purge is part of the mechanism. Stopping at this point is like giving up on a course of antibiotics three days in.
- Applying to damp skin. Moist skin absorbs tretinoin faster and more deeply, increasing irritation. Always wait 20 minutes after cleansing before applying.
- Skipping sunscreen. Tretinoin thins the stratum corneum and dramatically increases UV sensitivity. Daily SPF 50 is a non-negotiable part of the regimen, not a suggestion.
- Layering actives. Combining tretinoin with benzoyl peroxide, salicylic acid, glycolic acid, or vitamin C serum on the same night usually multiplies irritation. Space them out — tretinoin at night, gentler actives in the morning.
Can You Use Isotretinoin and Tretinoin Together?
It is not a routine combination, but it is not unheard of. Some dermatologists add topical tretinoin during the final weeks of an oral isotretinoin course — to aid post-inflammatory hyperpigmentation resolution and transition the patient to long-term maintenance. Others avoid it entirely because skin is already maximally dry and irritated during isotretinoin therapy.
If your clinician does combine them, expect the tretinoin to be started at 0.025% twice weekly and introduced no earlier than month 3 of the isotretinoin course. Always follow specific guidance from the prescriber — this is one area where DIY combining is a fast route to severe retinoid dermatitis.
Post-isotretinoin, about 10-25% of patients will eventually relapse and need maintenance. Many dermatologists use tretinoin alone (or with adapalene) as that maintenance, which also addresses any residual hyperpigmentation from the original acne.
Frequently Asked Questions
Is isotretinoin the same as tretinoin?
No — they share a name root but are different drugs. Isotretinoin is an oral capsule (13-cis-retinoic acid) used for severe acne. Tretinoin is a topical cream or gel (all-trans-retinoic acid) used for mild-to-moderate acne, wrinkles, and pigmentation. Isotretinoin works systemically and needs blood monitoring; tretinoin works only where applied.
Which is stronger, isotretinoin or tretinoin?
Isotretinoin is far more powerful — it reduces acne lesions by up to 90% during a course and keeps most patients clear for years afterwards. Tretinoin is effective but incremental, reducing lesion counts by 40-60% over 12 weeks and requiring ongoing use. However, strength comes with stronger side effects, which is why isotretinoin is reserved for severe cases.
Can tretinoin cure acne?
Tretinoin controls acne while you use it, but it does not offer a “cure” the way a completed isotretinoin course often does. Most people need to continue tretinoin indefinitely to keep breakouts at bay. That said, many patients find it sufficient for long-term management and appreciate having no systemic monitoring or dietary restrictions.
How long does isotretinoin take to work compared to tretinoin?
Isotretinoin typically takes 8 to 12 weeks before visible improvement, with peak results at 4 to 6 months. About a quarter of patients get worse in weeks 2 to 6 before improving. Tretinoin shows visible change in 4 to 12 weeks, with the full anti-acne benefit at 3 to 4 months and continuing texture and pigment improvements out to 12 months.
Can I use tretinoin while on isotretinoin?
Only under direct dermatologist supervision. Isotretinoin already maximally dries and thins the skin, so adding topical tretinoin early in the course usually causes severe irritation. Some clinicians add it toward the end of the course for pigmentation or maintenance. Never combine them without explicit prescriber approval.
Is tretinoin safer than isotretinoin?
Yes, in terms of systemic risk. Tretinoin’s side effects are localised — redness, peeling, dryness — and resolve quickly on stopping. Isotretinoin has rare but real systemic risks including lipid changes, liver enzyme elevations, and severe birth defects if used in pregnancy. Both are avoided in pregnancy, but only isotretinoin requires formal pregnancy-prevention programmes.
Does tretinoin help acne scars?
Tretinoin can meaningfully improve the appearance of shallow post-acne scars and is very effective for post-inflammatory hyperpigmentation (the dark marks left behind). For deeper atrophic scars — icepick, boxcar, rolling scars — tretinoin is usually combined with procedures such as microneedling, subcision, or laser resurfacing for best effect.
Will I need to go back on treatment after an isotretinoin course?
About 70-85% of patients remain acne-free for years after finishing a full isotretinoin course. Roughly 10-25% relapse within five years and may need a second course or a topical maintenance regimen — typically tretinoin or adapalene. Factors associated with relapse include young age at first course, female sex, hormonal acne patterns, and sub-therapeutic cumulative dose.
The Bottom Line
Isotretinoin and tretinoin occupy very different roles in dermatology despite sounding almost identical. Isotretinoin is the heavy artillery — reserved for acne severe enough to scar or refractory enough to resist everything else, with clear risks that demand monitoring and pregnancy prevention, but with a realistic chance of multi-year remission from a single 4-to-6-month course.
Tretinoin is the daily workhorse — gentler, cheaper, broader in its indications, and equally well-suited to the 25-year-old battling comedones as to the 45-year-old softening early wrinkles. It demands consistency, patience, and SPF, but the pay-off builds quietly month after month.
Neither drug is “better” in the abstract. The right choice is the one matched to your acne severity, risk tolerance, treatment history, and life circumstances — decided with a qualified dermatologist who has seen your skin in person. If you are considering either, browse our acne treatment range at MedsBase, or read our pillar guide covering everything you need to know about acne.
⚕️ Medical Disclaimer. This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Isotretinoin and tretinoin are prescription medications that require evaluation by a qualified healthcare professional. Never start, stop, or combine retinoid therapies without speaking to your doctor — particularly if you are pregnant, planning pregnancy, breastfeeding, or taking other medications. Always follow the guidance on your prescription and the advice of a licensed clinician.
Last updated: 2026-04-17 · Reviewed by MedsBase Clinical Content Team.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.