







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.

Reviewed by the MedsBase Editorial Team · Last updated: April 17, 2026
The World Health Organization estimates that more than 1.5 billion people — nearly a fifth of humanity — are infected with at least one soil-transmitted helminth, most of them in tropical and subtropical regions with limited sanitation. The two drugs that do most of the heavy lifting against these infections are ivermectin vs albendazole — two molecules that show up in nearly every mass drug administration program, every traveller’s medicine kit, and every parasitology textbook.
They’re often talked about interchangeably as “antiparasitic medication”, but they’re not the same drug — not even close. They work by completely different mechanisms, target different parasites, and excel in different situations. This guide walks through what each drug actually does, which infections each one treats best, and how clinicians decide between them in 2026.
- Ivermectin paralyses parasites by opening invertebrate nerve-cell chloride channels — effective against roundworms and ectoparasites, but not tapeworms.
- Albendazole starves parasites by disrupting their microtubules — effective against roundworms, tapeworms, and tissue-stage larvae.
- Both are on the WHO Essential Medicines List and are usually cheap and well-tolerated.
- Ivermectin is the go-to for scabies, lice, strongyloides, and onchocerciasis.
- Albendazole is the go-to for hookworm, ascaris, whipworm, tapeworms, and hydatid disease.
- For combined or mixed infections, many clinicians use both drugs in sequence or together.
Ivermectin vs Albendazole — Which Antiparasitic Actually Works Better in 2026?
What Are Ivermectin and Albendazole?
Quick Answer — What is Ivermectin vs Albendazole?
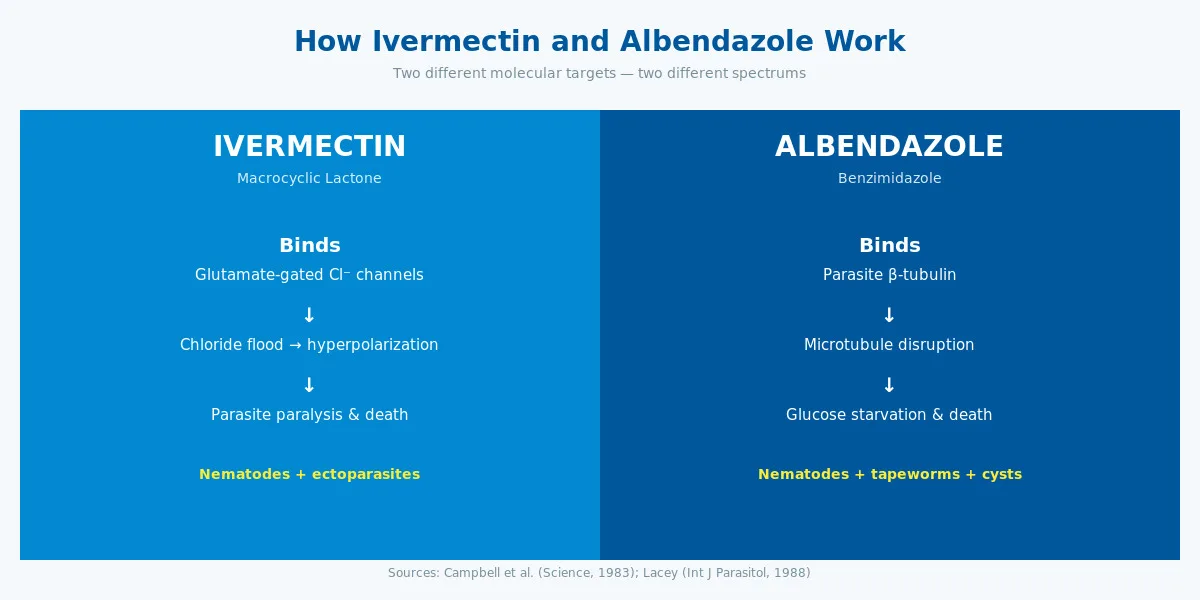
Ivermectin and albendazole are both prescription antiparasitic medicines, but they belong to different drug classes and target different parasites. Ivermectin is a macrocyclic lactone that paralyses nematodes and ectoparasites by opening glutamate-gated chloride channels. Albendazole is a benzimidazole that kills parasites by disrupting their microtubules. They’re complementary, not interchangeable.
Ivermectin was discovered in 1974 at Merck by William C. Campbell and Satoshi Ōmura, working from avermectin compounds produced by a single soil-dwelling bacterium — Streptomyces avermitilis — collected near a golf course in Japan. The human formulation was approved in 1987. Campbell and Ōmura shared the 2015 Nobel Prize in Physiology or Medicine for the discovery, which has since prevented tens of millions of cases of river blindness in sub-Saharan Africa.
Albendazole was first synthesised in 1972 at SmithKline Beecham and approved for human use in the mid-1980s. It belongs to the benzimidazole class — a family of anthelmintics that also includes mebendazole (sold as Mebex on MedsBase) and fenbendazole. All benzimidazoles work on the same molecular target but differ in spectrum and bioavailability.
Both drugs appear on the WHO Essential Medicines List and are distributed in huge volumes through mass drug administration (MDA) programs — more than a billion doses of ivermectin have been donated through the Mectizan Donation Program since 1987. In fact, ivermectin is arguably the single most consequential antiparasitic ever developed: it’s credited with preventing an estimated 40,000 cases of blindness every year across formerly hyperendemic regions of sub-Saharan Africa and Latin America, and driving onchocerciasis transmission to near-elimination in six countries.
Albendazole’s global impact is harder to headline but equally vast. The WHO estimates that school-age deworming programs — delivering 400 mg albendazole to hundreds of millions of children annually — are among the highest-impact public-health interventions ever measured, in terms of both health and educational outcomes per dollar spent. The drug’s simplicity (one tablet, flat dose, no refrigeration) is a large part of why.
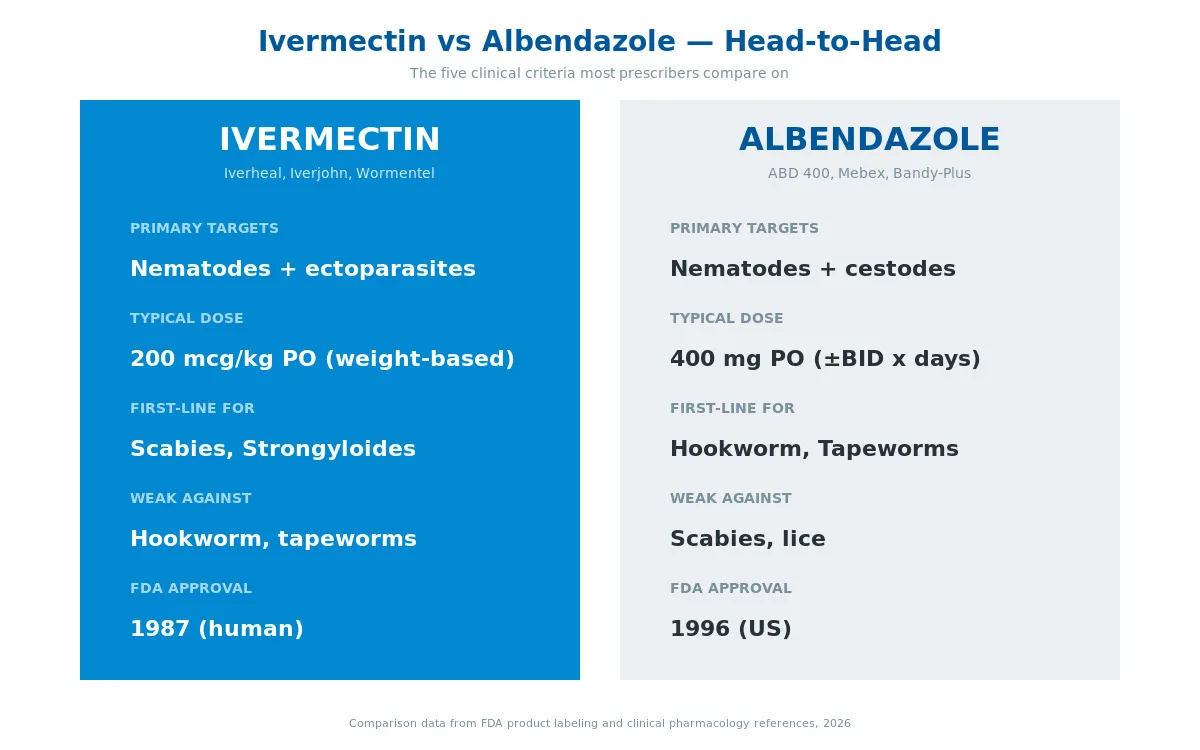
On MedsBase, ivermectin is sold under brands including Iverheal, Iverjohn, Wormentel, Ivimec, Neomec, and Ziverdo Kit. Albendazole is sold under ABD 400, Mebex, Bandy-Plus, Bendex, and Beworm Plus.
A brief history of broad-spectrum antiparasitics
Before the 1970s, anthelmintic therapy was a compromised affair — drugs like piperazine, diethylcarbamazine, and tetrachlorethylene were effective but carried significant toxicity or narrow coverage. Benzimidazoles changed that by offering a broad, low-toxicity option that worked against the most common roundworms. Ivermectin then added the missing piece — treating infections like onchocerciasis and strongyloides that benzimidazoles handled poorly.
The two drugs are effectively complementary rather than competitive. Mass drug administration programs targeting lymphatic filariasis famously combine them — ivermectin kills circulating microfilariae, while albendazole attacks both adult worms and any co-infecting intestinal nematodes in one go.
How Do Ivermectin and Albendazole Work?
Although both are classified as anthelmintics, they attack parasites through completely different molecular mechanisms. This is the single most important difference between them and explains why each excels at different infections.
Ivermectin — paralysis via chloride channels
Ivermectin binds with very high affinity to glutamate-gated chloride channels (GluCl) that exist in the nerve and muscle cells of invertebrates. When ivermectin locks onto these channels, it holds them open, flooding the cell with chloride ions. The parasite’s nerve and muscle cells become hyperpolarised and can no longer fire. Result: paralysis, starvation, and death.
Crucially, these specific chloride channels do not exist in humans or other mammals — we use different receptor systems for nerve transmission. That’s the basis of ivermectin’s wide therapeutic window in mammals.
Ivermectin also interacts with GABA-gated chloride channels, which adds to its paralytic effect. In mammals, GABA channels exist but are protected behind the blood-brain barrier — ivermectin doesn’t cross it at therapeutic doses, which is why it’s safe for oral use in people.
Albendazole — starvation via tubulin disruption
Albendazole takes a completely different approach. It binds to β-tubulin, a protein building block of the microtubule network inside parasite cells. Without functioning microtubules, the parasite loses its ability to transport glucose and other nutrients across cell membranes. Glycogen depletes, ATP production collapses, and the parasite starves.
Because albendazole binds preferentially to parasite β-tubulin (which differs structurally from mammalian β-tubulin), it selectively disrupts parasite energy metabolism while largely sparing the host.
These two mechanisms aren’t just academically interesting — they explain the spectrum of activity. Tapeworms and cyst-forming larvae depend heavily on tubulin-mediated nutrient uptake, so albendazole works wonders. Scabies mites and roundworms have the glutamate-chloride channel network that ivermectin exploits. Each drug has organisms it simply doesn’t touch.
What about resistance?
Drug resistance is a growing concern in veterinary parasitology, where benzimidazoles have been used at industrial scale in livestock for decades. In human medicine, benzimidazole resistance remains uncommon but has been documented in populations exposed to repeated mass drug administration. Single-nucleotide changes in parasite β-tubulin can reduce albendazole binding by 10-fold or more — the same mutation seen in sheep and cattle.
Ivermectin resistance is less well-established in human helminths, but has been reported in isolated onchocerciasis populations in West Africa after 20+ years of annual MDA. WHO monitoring programs now track parasite response over time, and combination therapy (ivermectin + albendazole) is partly intended to slow the emergence of resistance on either side.
For individual patients, resistance is rarely the explanation for treatment failure. Far more often the problem is misdiagnosis (treating the wrong parasite), suboptimal dosing, poor compliance, or rapid reinfection in endemic settings.
Key Uses & Applications
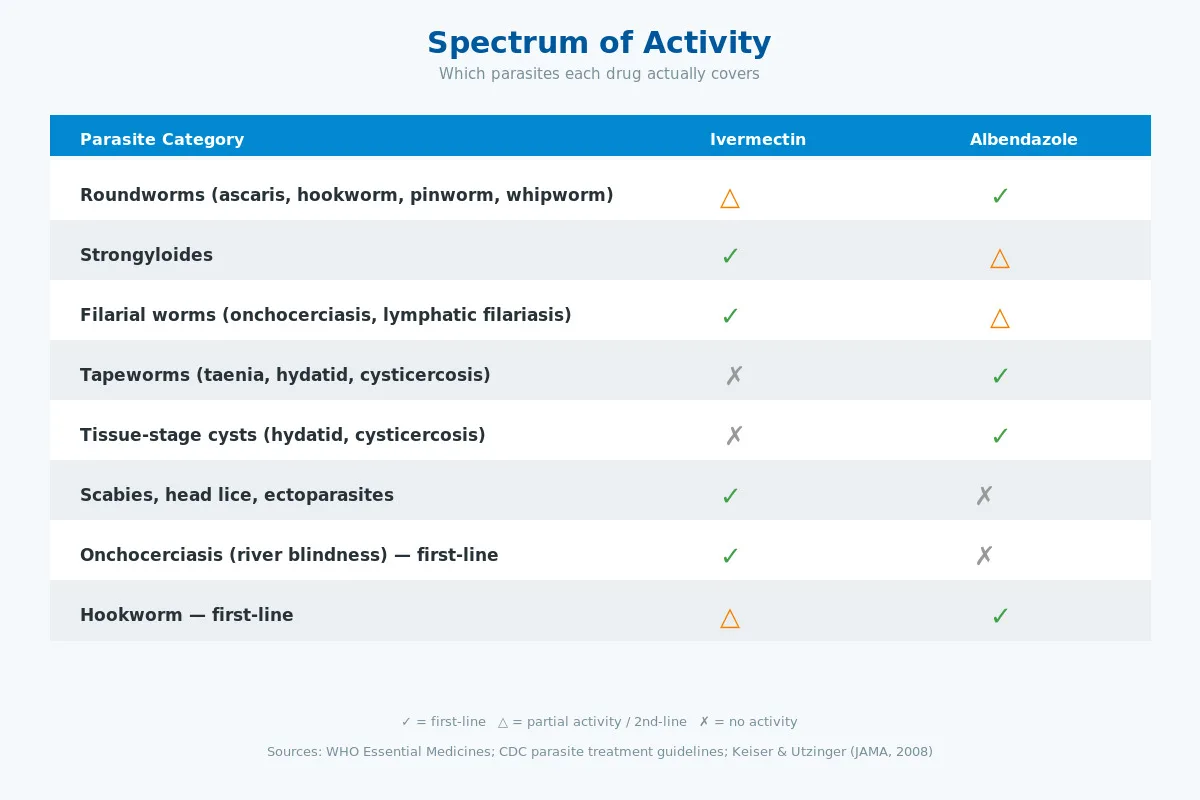
Infographic summary: Roundworms (ivermectin partial, albendazole first-line) · Strongyloides (ivermectin first-line, albendazole partial) · Filarial worms (ivermectin first-line) · Tapeworms & cysts (albendazole only) · Scabies / lice / ectoparasites (ivermectin only) · Onchocerciasis (ivermectin first-line) · Hookworm (albendazole first-line).
Both drugs have FDA-approved indications plus a larger universe of well-evidenced off-label uses. Here’s where each one shines.
Ivermectin
Strongyloidiasis — FDA-approved. Single 200 mcg/kg oral dose, repeated after 2 weeks if needed. Ivermectin is the unambiguous first-line treatment; albendazole works but is less reliable.
Onchocerciasis (river blindness) — FDA-approved. 150 mcg/kg every 6–12 months kills the microfilariae circulating in skin and eyes. Does not kill adult worms but drastically reduces transmission and prevents blindness.
Scabies — Off-label but well-established. 200 mcg/kg PO, repeated after 1 week. Ivermectin is the treatment of choice for crusted scabies and for institutional outbreaks where topical permethrin is impractical.
Head lice — Off-label oral therapy (200–400 mcg/kg PO, repeat after 7–10 days) when topical treatments fail.
Lymphatic filariasis (mass drug administration) — Combined with albendazole and sometimes diethylcarbamazine in WHO MDA programs.
Rosacea (topical) — 1% topical ivermectin cream (Soolantra) is FDA-approved for papulopustular rosacea, likely through an anti-inflammatory effect on Demodex mites.
Albendazole
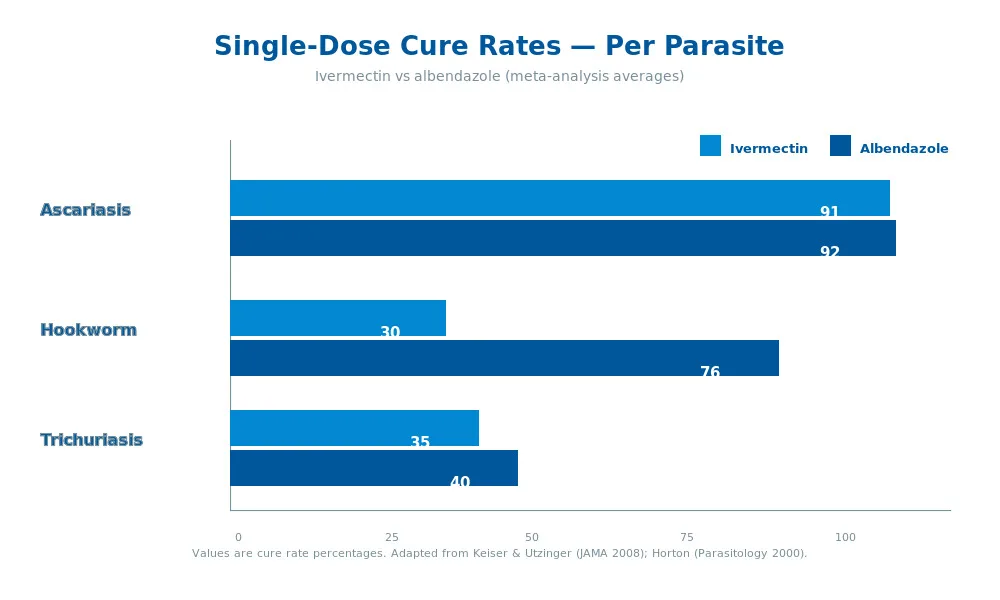
Ascariasis (roundworm) — 400 mg single dose. >90% cure rate.
Hookworm (Ancylostoma, Necator) — 400 mg single dose, sometimes repeated. Ivermectin is notably weak against hookworm — albendazole is the strongly preferred choice.
Enterobiasis (pinworm) — 400 mg single dose, repeat after 2 weeks. See our detailed guide on how albendazole helps in hookworm infection.
Trichuriasis (whipworm) — 400 mg daily for 3 days. Both drugs are modestly effective here; combination therapy improves cure rates.
Hydatid disease (cystic echinococcosis) — FDA-approved. 400 mg BID for up to 28-day cycles, often with surgery.
Neurocysticercosis — FDA-approved. 15 mg/kg/day in two divided doses for 8–30 days, usually with corticosteroids.
Taeniasis (tapeworm) — Praziquantel is often first-line, but albendazole is a well-established second-line option.
Giardiasis — Effective alternative to metronidazole in some protocols.
Safety Profile, Side Effects & Dosage
Both drugs are extraordinarily well-tolerated at standard single-dose courses. Serious adverse events are rare.
Common and Rare Side Effects
| Side effect | Drug(s) | Frequency | Severity |
|---|---|---|---|
| Nausea, abdominal pain | Both | Common (5–15%) | Mild |
| Headache | Both | Common (5–10%) | Mild |
| Dizziness | Both | Uncommon (2–5%) | Mild |
| Diarrhoea | Both | Uncommon (2–5%) | Mild |
| Rash / pruritus | Both | Uncommon (1–3%) | Mild |
| Reversible hair loss | Albendazole (long use) | Uncommon | Mild |
| Elevated liver enzymes | Albendazole | Common in long courses | Monitor |
| Bone marrow suppression | Albendazole | Rare in long courses | Serious — monitor CBC |
| Mazzotti reaction (in active onchocerciasis) | Ivermectin | Common in active infection | Usually mild |
| Encephalopathy (Loa loa co-infection) | Ivermectin | Rare | Serious — screen in endemic areas |
When to monitor
- Albendazole courses lasting more than 7–10 days (neurocysticercosis, hydatid disease) require baseline and periodic liver function tests (LFTs) and complete blood counts (CBCs).
- Ivermectin used in Loa-endemic regions (parts of Central Africa) requires screening for high Loa microfilaria loads before a first dose, because rapid die-off can trigger fatal encephalopathy.
Drug Interactions
- Albendazole levels rise with cimetidine, praziquantel, and fatty meals (desired for cyst-disease dosing).
- Ivermectin is metabolised mostly by CYP3A4; strong inhibitors (ketoconazole, ritonavir) and inducers (rifampicin) can alter its levels modestly but rarely require dose change.
Pregnancy and Breastfeeding
Albendazole is category C and generally avoided in the first trimester due to teratogenicity in animal studies. Used later in pregnancy only when the maternal benefit clearly justifies the risk. Ivermectin has a similar caution. Both drugs have been given unintentionally during MDA campaigns to pregnant women without consistent evidence of harm, but the default is to defer until after delivery. Always consult a prescriber — never self-treat parasitic infections in pregnancy.
What Does the Research Say?
The evidence base for both drugs is enormous. Here are the landmark studies every practitioner should know.
| Study | Year | Finding | Source |
|---|---|---|---|
| Campbell et al. | 1983 | Ivermectin efficacy against onchocerciasis; established 150 mcg/kg single-dose paradigm | Science |
| Horton | 2000 | Albendazole cure rates: ascaris >90%, hookworm 70–80%, pinworm ~100% | Parasitology |
| Keiser & Utzinger | 2008 | Meta-analysis: albendazole outperforms mebendazole and ivermectin for hookworm cure rates | JAMA |
| Romani et al. | 2015 | Mass drug administration with ivermectin reduced scabies prevalence from 32% to 2% in Fiji | NEJM |
| Buonfrate et al. | 2019 | Single-dose ivermectin well tolerated in >100,000 MDA recipients | PLOS NTDs |
Research suggests ivermectin’s efficacy in strongyloides exceeds that of albendazole — cure rates of 95%+ vs 45–85% for albendazole across multiple studies. For scabies, ivermectin’s convenience (oral single dose) combined with permethrin-comparable cure rates is why it’s overtaken topical treatment in outbreak settings.
Early studies indicate the combination of ivermectin plus albendazole is more effective than either drug alone for mixed soil-transmitted helminth infections — a finding that drives the WHO-recommended MDA strategy in high-burden regions. See our related guide on parasite cleanse evidence for the broader context.
The fenbendazole vs ivermectin conversation — popular in self-medicating circles — is covered separately in our fenbendazole vs ivermectin comparison. And for a broader primer on ivermectin specifically, see our ivermectin complete guide.
Ivermectin vs Albendazole — Head-to-Head Comparison
| Criterion | Ivermectin | Albendazole |
|---|---|---|
| FDA approval year | 1987 (human) | 1996 (US for hydatid & cysticercosis) |
| Drug class | Macrocyclic lactone | Benzimidazole |
| Molecular target | Glutamate-gated Cl⁻ channels | β-tubulin |
| Primary spectrum | Nematodes + ectoparasites | Nematodes + cestodes + larval cysts |
| Tapeworm coverage | No | Yes |
| Scabies / lice coverage | Yes | No |
| Onchocerciasis | First-line | Not used |
| Strongyloides | First-line | Alternative |
| Hookworm | Weak | First-line |
| Pinworm, ascaris | Effective | First-line (classic) |
| Cysticercosis / hydatid | No | First-line |
| Typical adult dose | 200 mcg/kg PO | 400 mg PO (±BID) |
| Dosing frequency | Usually single dose | Single dose to 28-day cycles |
| Food interaction | Take on empty stomach (label) | Take with fatty meal (5x absorption) |
| Long-course safety | Excellent | Requires LFT + CBC monitoring |
| Generic cost | Very low | Very low |
| Pregnancy | Generally avoided | Generally avoided in T1 |
Bottom line: ivermectin is the antiparasitic of choice for strongyloides, onchocerciasis, scabies, and lice. Albendazole is the antiparasitic of choice for hookworm, ascaris, pinworm, tapeworms, and tissue-larval infections. The two drugs overlap on some roundworm indications but diverge sharply at the edges of each spectrum. Neither is “stronger” — they simply hit different targets.
How to Take Ivermectin or Albendazole Correctly
Four universal rules apply:
- Weigh first (especially for ivermectin). Ivermectin is dosed by body weight (150–200 mcg/kg) — getting the dose right matters more than for albendazole’s flat 400 mg.
- Take albendazole with a fatty meal. Albendazole absorption jumps roughly 5x when taken with fat. Milk, yogurt, peanut butter, or an avocado will do. Ivermectin is label-recommended on an empty stomach but recent data suggests food has minimal impact.
- Complete the course. Single-dose therapies often need a follow-up dose at 1–2 weeks to catch any parasites that hatched after the first treatment. Extended courses (hydatid, neurocysticercosis) must not be stopped early.
- Retest for strongyloides. Strongyloides autoinfection is insidious — confirm cure with a follow-up stool test or serology 4–6 weeks after treatment, especially in immunocompromised patients.
Practical tips
- Don’t split ivermectin tablets unless weight-dose math requires it.
- Store both drugs at room temperature, away from moisture.
- Avoid alcohol during albendazole long courses (liver load).
- Watch for visual changes on long-course albendazole — a rare but documented side effect.
Browse our full antiparasitic range — including Wormentel, Iverheal, Iverjohn, ABD 400 (Albendazole), Mebex, and Bandy-Plus — all shipped discreetly worldwide.
Frequently Asked Questions
Is ivermectin stronger than albendazole?
Neither drug is universally “stronger” — they’re simply active against different parasite families. Ivermectin excels at strongyloides, onchocerciasis, scabies, and lice. Albendazole excels at hookworm, ascaris, tapeworms, and tissue-stage cysts like hydatid disease. Clinicians choose based on the specific diagnosis, not on raw potency.
Can I take ivermectin and albendazole together?
Yes — the combination is routinely used in WHO mass drug administration programs targeting lymphatic filariasis and mixed soil-transmitted helminth infections. Ivermectin handles microfilariae, strongyloides, and ectoparasites; albendazole handles tapeworms, hookworm, and whipworm. The pairing is well-tolerated and often more effective than either drug alone in mixed infections — but should only be combined under medical supervision.
Does ivermectin kill tapeworms?
No — ivermectin has very limited activity against cestodes (tapeworms). Its mechanism targets glutamate-gated chloride channels that tapeworms don’t rely on the same way roundworms and ectoparasites do. For tapeworm infections like taeniasis, cysticercosis, or hydatid disease, albendazole or praziquantel is the correct choice.
Which is better for a worm infection in children?
For pinworm, ascaris, or hookworm in children over 2, albendazole 400 mg single dose is the standard. Ivermectin is used in children weighing over 15 kg, mostly for scabies, lice, or strongyloides. Paediatric treatment should always be supervised by a prescriber because dosing, co-existing conditions, and the specific parasite all affect the choice.
How fast does albendazole kill parasites?
Albendazole starts disrupting parasite metabolism within hours of absorption, but visible results — like worm expulsion in stool — typically take 24–72 hours. Complete parasite clearance for most intestinal helminths is achieved within a week. For tissue-stage infections like neurocysticercosis or hydatid disease, treatment is measured in weeks to months with imaging follow-up.
Is ivermectin safe for long-term use?
Single or repeated doses months apart (as used in onchocerciasis MDA) have an excellent long-term safety record — more than a billion doses have been administered through the Mectizan program since 1987. Continuous daily ivermectin is not a standard protocol and has not been studied at that cadence. Most legitimate indications require only single or infrequent dosing.
Do I need a prescription for ivermectin or albendazole?
Yes. In virtually every country, both drugs are prescription-only for human use. Self-prescribing risks missing the actual diagnosis (many “parasite” symptoms aren’t parasites at all) and using the wrong drug for the specific organism. A proper work-up — stool microscopy, antigen testing, or serology — should precede treatment.
Which drug has fewer side effects?
At standard short courses, both drugs are extremely well-tolerated. The main difference: albendazole’s long courses (used for hydatid or neurocysticercosis) can cause reversible hair loss, liver enzyme elevation, and rarely bone marrow suppression, so they require lab monitoring. Ivermectin’s main safety concern is the Mazzotti reaction in active onchocerciasis and the encephalopathy risk in patients with high Loa loa microfilaraemia.
The Bottom Line
Ivermectin vs albendazole is the wrong framing in most cases — the right question is “which parasite do we have, and which drug covers it best?”. Albendazole is the broader, older workhorse: roundworms, tapeworms, and tissue cysts. Ivermectin is the more specialised tool: ectoparasites, strongyloides, onchocerciasis, and scabies.
For most travellers and most common intestinal worm infections, albendazole is the first drug most clinicians reach for. For scabies, lice, or a confirmed strongyloides infection, ivermectin wins. For complex mixed infections, combining both under medical supervision is routine practice.
Decision summary — how most prescribers actually choose
- Travel-related roundworm infection (ascaris, hookworm): albendazole 400 mg single dose.
- Pinworm in a child: albendazole 400 mg single dose, repeat at 2 weeks.
- Scabies (adult or institutional outbreak): ivermectin 200 mcg/kg PO, repeat at 1 week.
- Suspected strongyloides: ivermectin 200 mcg/kg, confirm cure with serology at 6 weeks.
- Hydatid cyst / neurocysticercosis: albendazole long course (weeks to months) with monitoring.
- Mass drug administration (WHO programs): ivermectin + albendazole in combination.
Whichever drug you end up on, the golden rules are the same: confirm the diagnosis, follow the dose schedule, take albendazole with fat, and retest if strongyloides is in the differential.
Ready to explore your options? Browse our antiparasitic range or speak to your healthcare provider about which regimen fits your situation.
Last medical review: April 2026. Next scheduled review: October 2026.
Authoritative references: WHO soil-transmitted helminthiases fact sheet · Mectizan Donation Program · CDC Parasites A-Z · Keiser J, Utzinger J. Efficacy of Current Drugs Against Soil-Transmitted Helminth Infections: Systematic Review and Meta-analysis. JAMA. 2008;299(16):1937-1948.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.