







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
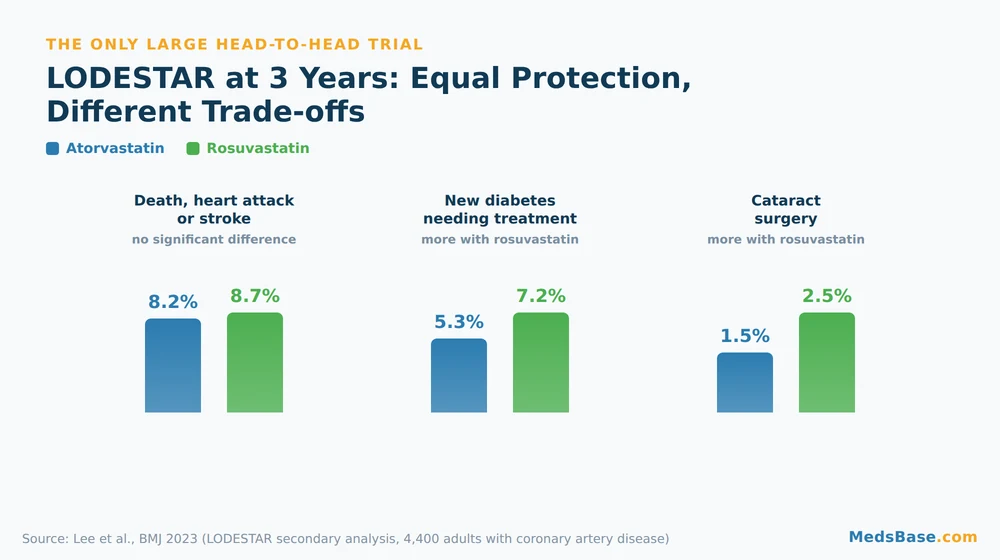
When researchers finally ran the head-to-head trial everyone wanted — 4,400 adults with coronary artery disease, three years, rosuvastatin against atorvastatin — the stronger statin did not win. Death, heart attack or stroke happened in 8.7% of the rosuvastatin group and 8.2% of the atorvastatin group. Statistically, a tie.
That result reframes the whole atorvastatin vs rosuvastatin question. If the more potent drug does not deliver more protection, then “which statin is stronger?” is the wrong thing to ask. This guide covers what the trials actually found, why 10 mg of one is not 10 mg of the other, the interaction split that decides the choice for many people, and the honest trade-offs each drug carries.
One of those trade-offs surprised even the trial investigators — we will get to it in the research section.
Key takeaways
- Rosuvastatin lowers LDL about 8% more than atorvastatin across matched doses — but that extra potency did not translate into fewer heart attacks.
- Milligrams are not interchangeable: 10 mg of atorvastatin is roughly 5 mg of rosuvastatin. Getting this wrong is the most common switching error.
- The head-to-head trial found rosuvastatin came with more new-onset diabetes and more cataract surgery — the numbers are in the research section.
- Your other medications often pick the winner, because the two drugs are cleared by completely different routes.
- If you stopped a statin over muscle aches, a landmark trial suggests the drug may not have been the cause — covered in the side-effects section.
- Both are FDA-approved, both are available as low-cost generics, and both work best when you actually keep taking them.

Atorvastatin vs Rosuvastatin: What’s the Difference?
Atorvastatin and rosuvastatin are both statins — HMG-CoA reductase inhibitors that lower LDL (“bad”) cholesterol and reduce the risk of heart attack and stroke. The core difference is potency and chemistry: rosuvastatin lowers LDL more per milligram and is water-loving, while atorvastatin is fat-loving and carries the longer clinical track record.
Atorvastatin arrived first and became one of the most-prescribed medicines in history under the brand name Lipitor. Rosuvastatin followed as a deliberately more potent molecule, best known as Crestor. Both are now widely available as inexpensive generics from WHO-GMP-certified manufacturers, which is why the choice between them is a clinical question rather than a budget one.
Here is what most comparison pages get wrong. They present this as a contest with a winner. It isn’t. Both qualify as a high-intensity statin at the right dose, both have large outcome trials behind them, and the honest answer for most people is that either would work. What decides it is your LDL target, your other medications, and your kidneys — not a leaderboard.
What they have in common
More unites these two drugs than separates them:
- Both block the same liver enzyme and lower LDL by the same mechanism.
- Both are proven to reduce cardiovascular events in large randomised trials.
- Both are taken once daily as a tablet, long-term.
- Both share the statin side-effect profile — muscle aches, rare liver enzyme changes, a small diabetes signal.
- Neither works if it sits in the cupboard. Adherence beats potency, every time.
How Atorvastatin vs Rosuvastatin Work (The Science, Simply)
Both statins work by blocking HMG-CoA reductase, the liver enzyme that manufactures cholesterol. Starved of its own supply, the liver pulls more LDL out of your bloodstream to compensate. Blood LDL falls, and with it your long-term risk of heart attack and stroke.
Think of your liver as a warehouse that both makes cholesterol and imports it. Statins shut down the factory floor. The warehouse still needs stock, so it opens more loading bays — LDL receptors — and starts pulling cholesterol in from the blood. That second step is what actually lowers your numbers.

So if the mechanism is identical, where does the difference come from? Two places: how tightly each molecule binds the enzyme, and how it moves around your body.
Rosuvastatin binds more tightly and lingers longer. It has a half-life of about 19 hours versus roughly 14 for atorvastatin, and it produces more binding interactions with the target enzyme. That is the pharmacology behind its per-milligram edge.
Atorvastatin is lipophilic; rosuvastatin is hydrophilic. Fat-loving atorvastatin diffuses passively into cells throughout the body. Water-loving rosuvastatin needs transporter proteins to get into liver cells, which makes it more liver-selective — but also more dependent on those transporters working normally. This single chemical difference drives most of the interaction differences discussed later.
Statin Equivalent Dose — Why 10 mg Isn’t Always 10 mg
Rosuvastatin is roughly twice as potent as atorvastatin milligram for milligram. Rosuvastatin 5 mg lowers LDL about as much as atorvastatin 10 mg, and rosuvastatin 20 mg roughly matches atorvastatin 40 mg. Comparing the two by dose number alone is the single most common mistake people make.
This trips up more people than any other part of the comparison. Someone moves from atorvastatin 40 mg to rosuvastatin 40 mg thinking it is a like-for-like swap, and they have actually roughly doubled their statin intensity. Someone else drops from atorvastatin 20 mg to rosuvastatin 5 mg, sees a smaller number, and assumes they have been downgraded — when the LDL effect is nearly the same.
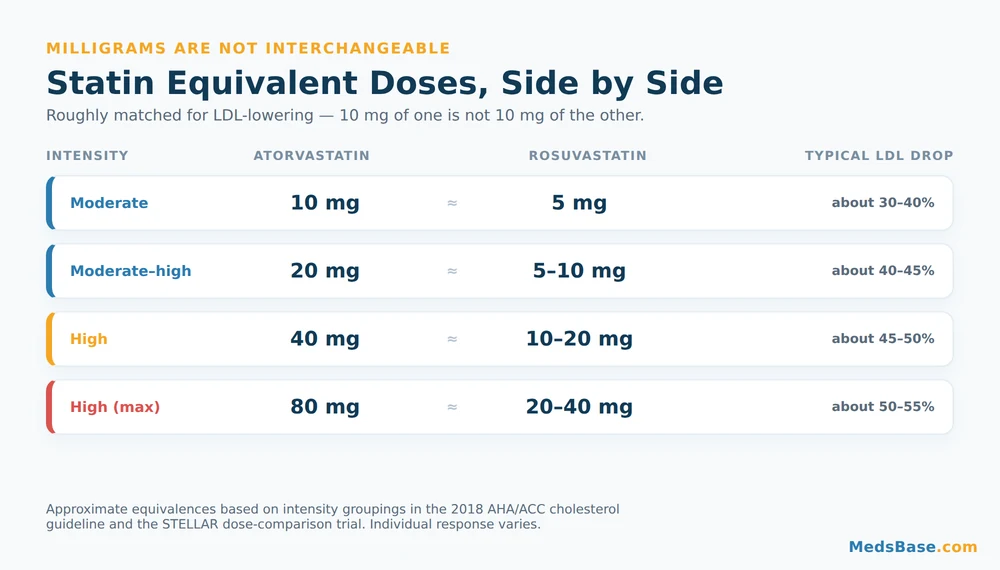
Guidelines sidestep the confusion by grouping statins into intensity tiers rather than doses. The 2018 American College of Cardiology and American Heart Association cholesterol guideline defines a high-intensity statin as anything that lowers LDL by 50% or more — which means atorvastatin 40–80 mg or rosuvastatin 20–40 mg. Both drugs reach the top tier; rosuvastatin just needs fewer milligrams to get there. Use the statin equivalent dose table below to match them properly.
| Intensity tier | Atorvastatin | Rosuvastatin | Typical LDL reduction |
|---|---|---|---|
| Moderate | 10 mg | 5 mg | About 30–40% |
| Moderate–high | 20 mg | 5–10 mg | About 40–45% |
| High | 40 mg | 10–20 mg | About 45–50% |
| High (maximum) | 80 mg | 20–40 mg | About 50–55% |
Two caveats worth knowing. First, statin dose-response is famously flat — the rule of 6 holds that each doubling of the dose buys only about 6% more LDL reduction. Going from 20 mg to 40 mg is not twice the effect; it is a modest bump. Second, these equivalences are population averages. Your own response can land well off the chart in either direction, which is why the follow-up blood test matters more than the number on the tablet.
Atorvastatin vs Rosuvastatin: Side Effects, Dosage and Safety
Both statins share a similar safety profile: muscle aches are the most-reported complaint, liver enzyme rises are uncommon and usually harmless, and serious muscle damage is rare. Rosuvastatin carries dose caps in severe kidney disease and for some people of Asian ancestry; atorvastatin generally does not need kidney-related adjustment. In short, statin side effects are broadly a class story rather than a reason to prefer one of these two drugs over the other.
Now for the honest part, because this is where a lot of health content either hides the risks or sensationalises them.
| Side effect | Frequency | Severity | What to do |
|---|---|---|---|
| Muscle aches or weakness | Common in practice (often not drug-caused — see below) | Mild to moderate | Tell your doctor; do not just stop. A re-challenge or dose change usually sorts it. |
| Headache, nausea, digestive upset | Common | Mild | Usually settles in the first weeks. Taking it with food can help. |
| Raised liver enzymes | Uncommon | Usually mild, reversible | Picked up on routine bloods; rarely needs stopping. |
| New-onset type 2 diabetes | Uncommon; slightly higher with rosuvastatin in one trial | Moderate — manageable | Worth discussing if you are already pre-diabetic. Benefits still outweigh this for most at-risk people. |
| Cataract surgery | Uncommon; slightly higher with rosuvastatin in one trial | Moderate — treatable | Mention any vision changes at your next review. |
| Protein or blood in urine (rosuvastatin, higher doses) | Uncommon | Usually transient | Flagged on urine tests; your doctor may check kidney function. |
| Rhabdomyolysis (severe muscle breakdown) | Rare | Serious — urgent | Seek medical help for severe muscle pain with dark urine. |
The muscle-ache question — and the trial that reframed it
Here is the finding that resolves the open loop from earlier, and it is genuinely counterintuitive.
The SAMSON trial (Wood et al., New England Journal of Medicine, 2020) recruited people who had already abandoned statins because of side effects. Each participant cycled through twelve one-month bottles in random order: four containing atorvastatin, four containing placebo, four containing nothing at all. Nobody knew which was which.
The symptom scores during statin months were not significantly different from the placebo months. The aches were real — people genuinely felt them — but they appeared just as strongly on a dummy tablet. Roughly half the participants went on to successfully restart a statin.
This does not mean statin side effects are imaginary — muscle symptoms do happen, and they matter. It means that if you switched from atorvastatin to rosuvastatin hoping to escape aches, the swap may not be the variable that helps. Pharmacists see this pattern constantly: the person is convinced drug A caused the problem, drug B feels fine for a month, and then the same aches return. Worth discussing honestly with your doctor before assuming the molecule is the culprit.
Who should avoid these statins
Who is this for? Who should avoid it?
Likely a good fit: adults with raised LDL cholesterol, established heart disease, diabetes with cardiovascular risk factors, or a calculated 10-year risk that puts them in a treatment tier. Also anyone who has had a heart attack or stroke — the evidence here is about as strong as it gets in medicine.
Should avoid or use extra caution: anyone who is pregnant, trying to conceive, or breastfeeding (statins are contraindicated); people with active liver disease; anyone with unexplained persistent muscle pain. Rosuvastatin specifically needs dose caps in severe kidney impairment and a lower starting dose for some people of Asian ancestry, who reach higher blood levels at the same dose. Heavy alcohol use raises the risk of liver-related problems with both drugs.
Always individual: if you take ciclosporin, certain HIV or hepatitis C antivirals, gemfibrozil, or clarithromycin, the choice between these two statins is not a coin flip — see the interactions section.
What Does the Research Say?
The evidence on rosuvastatin vs atorvastatin splits cleanly in two. On cholesterol numbers, rosuvastatin wins. On cardiovascular outcomes — the thing that actually matters — the two drugs are indistinguishable. Understanding that gap is the key to this whole comparison.
| Study | Year | What it found | Source |
|---|---|---|---|
| STELLAR (Jones et al.) | 2003 | Rosuvastatin lowered LDL a mean of 8.2% more than atorvastatin across the 10–80 mg range; HDL rose +7.7% to +9.6% vs +2.1% to +6.8% with other statins. | Am J Cardiol |
| SATURN (Nicholls et al.) | 2011 | Rosuvastatin 40 mg vs atorvastatin 80 mg over 2 years: plaque volume fell 1.22% vs 0.99% — no significant difference, despite lower LDL on rosuvastatin (62.6 vs 70.2 mg/dL). | N Engl J Med |
| SAMSON (Wood et al.) | 2020 | In people who had quit statins for side effects, symptom scores on atorvastatin were not significantly different from placebo; about half were able to restart therapy. | N Engl J Med |
| LODESTAR (Lee et al.) | 2023 | 4,400 adults with coronary artery disease over 3 years: death/heart attack/stroke 8.7% (rosuvastatin) vs 8.2% (atorvastatin) — no significant difference. Rosuvastatin: more new diabetes (7.2% vs 5.3%) and cataract surgery (2.5% vs 1.5%). | BMJ |
What this means for you: if your goal is hitting an LDL target that atorvastatin cannot reach, rosuvastatin has a real, measurable edge. If your goal is preventing a heart attack — and it usually is — the evidence says either drug at the right intensity gets you there.
Two important caveats keep this honest. LODESTAR was a secondary analysis, and its trade-off findings (the diabetes and cataract signals) came from an open-label design, so they are a signal worth knowing rather than settled fact. Other observational work has hinted at a small edge for rosuvastatin that mostly failed to reach statistical significance. The fair summary: the difference between these two drugs is smaller than the difference between taking one and not taking one.
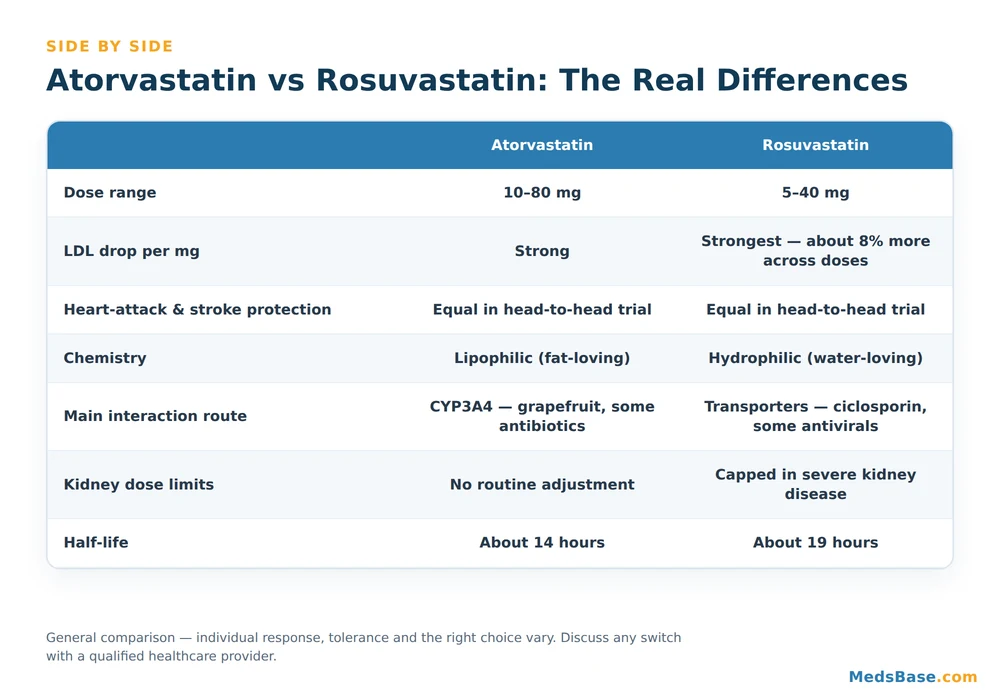
Atorvastatin vs Rosuvastatin — Head-to-Head Comparison
Here is where the two drugs genuinely diverge, stripped of the marketing.
| Criterion | Atorvastatin | Rosuvastatin |
|---|---|---|
| Dose range | 10–80 mg | 5–40 mg |
| LDL reduction per mg | Strong | Strongest — about 8% more across matched doses |
| Heart attack / stroke prevention | Equal in head-to-head trial | Equal in head-to-head trial |
| Chemistry | Lipophilic (fat-loving) | Hydrophilic (water-loving), more liver-selective |
| Main interaction route | CYP3A4 — grapefruit, some antibiotics, some antivirals | Transporters — ciclosporin, gemfibrozil, some antivirals |
| Severe kidney disease | No routine dose adjustment | Dose capped |
| Asian-ancestry dosing | Standard | Lower starting dose advised |
| Half-life | About 14 hours | About 19 hours |
| Timing | Any time of day | Any time of day |
Which one fits which situation? If you have severe kidney impairment, are on ciclosporin, or need the drug with the deepest outcome evidence base, atorvastatin is the more straightforward choice — and you can browse atorvastatin tablets at MedsBase across the full 10–80 mg range. If you are already at atorvastatin 80 mg and still above your LDL target, or you take a CYP3A4-heavy medication list, rosuvastatin earns its place; Crestor and its generic equivalents cover 5–20 mg. If neither gets you to target alone, adding ezetimibe to a moderate statin dose is often better tolerated than pushing either drug to its maximum.
What about other statins?
These two are not the only options. Simvastatin is older, cheaper and moderate-intensity, but it has more interactions than either drug here. Pravastatin is the gentlest on interactions and is sometimes chosen for people on complex regimens, at the cost of potency. Pitavastatin is a niche option worth knowing about if you have had trouble with both of the drugs in this guide — our guide to Livalo and pitavastatin covers where it fits. For the full landscape, see our roundup of the best cholesterol medications.
Drug Interactions — Where Atorvastatin vs Rosuvastatin Really Differ
This is the section that decides the choice for more people than potency ever does, and it is the one consumer guides skip. Atorvastatin is broken down by the CYP3A4 enzyme; rosuvastatin barely touches the CYP system and instead depends on liver transporter proteins. Different routes, different conflicts.
Atorvastatin’s watch list (CYP3A4)
Anything that blocks CYP3A4 raises atorvastatin levels, and higher levels mean higher muscle-related risk:
- Grapefruit juice in large amounts — the classic. An occasional glass is generally not the issue; daily litres are.
- Clarithromycin and some other macrolide antibiotics.
- Certain antifungals such as itraconazole and ketoconazole.
- Some HIV and hepatitis C antivirals.
- Amlodipine — a very common blood-pressure partner that mildly raises atorvastatin levels, which is why atorvastatin dose caps exist in some combinations.
Rosuvastatin’s watch list (transporters)
Rosuvastatin sidesteps the grapefruit problem entirely — but it has its own list:
- Ciclosporin — dramatically raises rosuvastatin levels; generally avoided together.
- Gemfibrozil — a fibrate that raises levels and muscle risk.
- Certain HIV antivirals, which can push rosuvastatin levels up sharply.
- Warfarin — both statins can nudge INR, so monitoring matters.
- Some antacids reduce absorption if taken at the same time; separate them by a couple of hours.
So here is the practical rule that falls out of this. If your medication list is heavy on CYP3A4 inhibitors, rosuvastatin is often the cleaner fit. If you take ciclosporin or gemfibrozil, atorvastatin usually is. Bring your full list — including supplements — to your pharmacist and let the interactions pick the drug. It is a five-minute conversation that outperforms any article, including this one.
How to Choose Between Atorvastatin vs Rosuvastatin — Practical Guidance
There is no universal winner. There is a right answer for you, and it usually falls out of three questions rather than a potency ranking.

- Know your LDL target and your gap. Ask what your current LDL is and where it needs to be. If you need a 50%+ drop, you need a high-intensity statin — atorvastatin 40–80 mg or rosuvastatin 20–40 mg. If you need 35%, a moderate dose of either is plenty.
- Audit your other medicines first. Run your list against the two interaction profiles above. This step alone settles the question for a large share of people.
- Check the constraints. Severe kidney impairment, Asian ancestry, pregnancy plans and liver history all change the calculus — and only rosuvastatin has ancestry- and kidney-based dose caps.
- Take it consistently, at any time of day. Both drugs have long enough half-lives that the old “statins must be taken at night” rule does not apply to them — that advice belongs to the short-acting statins. The best time is the time you will remember.
- Re-test at 4–12 weeks. A lipid panel after starting or changing dose is how you find out what your body actually did, versus what the population average predicted.
Mistakes to avoid
- Treating mg as mg when switching. Match on intensity tier, never on the number.
- Stopping without telling anyone because of aches. Given the SAMSON findings, a supervised re-challenge is worth trying first.
- Chasing the maximum dose for a 6% gain when adding ezetimibe would get you further with fewer side effects.
- Assuming a lower LDL number always means better protection. SATURN and LODESTAR both landed the same way: lower numbers on rosuvastatin, same outcomes.
- Ignoring the basics. No statin outruns smoking, and diet still moves the needle — our guide to high-cholesterol foods covers what genuinely matters.
Related reading
- Best cholesterol medications: 10 evidence-backed options — where statins sit among all the lipid-lowering classes.
- Livalo (pitavastatin) guide — the alternative worth knowing if you have struggled with both drugs here.
- Blood pressure medication for seniors — because cholesterol is rarely the only number being managed.
Frequently Asked Questions
Q: Which is better, atorvastatin or rosuvastatin?
A: Neither is universally better. On rosuvastatin vs atorvastatin, rosuvastatin lowers LDL cholesterol about 8% more at matched doses, but the large LODESTAR head-to-head trial found no difference in death, heart attack or stroke over three years. Atorvastatin has the longer outcome record and fewer transporter interactions; rosuvastatin is more potent per milligram and avoids the grapefruit and CYP3A4 problem. The better drug is the one that fits your LDL target, your other medications and your kidneys.
Q: Is 10 mg of rosuvastatin the same as 10 mg of atorvastatin?
A: No. Rosuvastatin is roughly twice as potent milligram for milligram, so rosuvastatin 10 mg is closer to atorvastatin 20 mg in LDL-lowering effect. Rosuvastatin 5 mg approximately equals atorvastatin 10 mg, and rosuvastatin 20 mg approximately equals atorvastatin 40 mg. Never swap between the two on dose number alone — match them by intensity tier instead, and confirm with a lipid panel a few weeks later.
Q: Can I switch from atorvastatin to rosuvastatin?
A: Yes, switching is common and straightforward, but the dose must be converted properly rather than carried across. Reasons to switch include not reaching your LDL target on a high atorvastatin dose, or a new medication that clashes with CYP3A4. Your doctor will pick an equivalent intensity and re-check your lipids in about 4–12 weeks. If you are switching because of muscle aches, be aware the symptoms may follow you — the SAMSON trial found most statin symptoms also occurred on placebo.
Q: Does rosuvastatin have more side effects than atorvastatin?
A: Broadly the two have similar side-effect profiles, with muscle aches leading the list for both. The LODESTAR trial did find more new-onset diabetes (7.2% vs 5.3%) and more cataract surgery (2.5% vs 1.5%) with rosuvastatin over three years. Those are real signals worth knowing, though they came from a secondary open-label analysis. Rosuvastatin also needs dose caps in severe kidney disease and a lower starting dose for some people of Asian ancestry.
Q: Which statin is safest for the kidneys?
A: Atorvastatin generally needs no routine dose adjustment for kidney function, while rosuvastatin is dose-capped in severe kidney impairment and can cause transient protein in the urine at higher doses. That makes atorvastatin the more straightforward option for people with significantly reduced kidney function. Neither drug is considered harmful to healthy kidneys, and statins are widely used in chronic kidney disease — the difference is in dosing care, not outright risk.
Q: Can I drink grapefruit juice with rosuvastatin?
A: Rosuvastatin does not have the grapefruit interaction, because it is barely metabolised by the CYP3A4 enzyme that grapefruit blocks. Atorvastatin does go through CYP3A4, so large or daily quantities of grapefruit juice can raise its levels and muscle-related risk. If grapefruit is a fixed part of your routine, that is a genuine point in rosuvastatin’s favour — but check the rest of your medication list before switching for that reason alone.
Q: Do I have to take these statins at night?
A: No. The “take it at night” rule applies to short-acting statins such as simvastatin, because the liver makes most of its cholesterol overnight. Atorvastatin has a half-life of about 14 hours and rosuvastatin about 19 hours — long enough to cover a full 24-hour cycle whenever you take them. Pick the time you are most likely to remember consistently, because missed doses cost you far more than timing ever will.
Q: What if neither statin gets my cholesterol to target?
A: Adding a second drug with a different mechanism usually beats maximising the statin dose, because of the rule of 6 — each doubling buys only about 6% more LDL reduction. Ezetimibe, which blocks cholesterol absorption in the gut, is the usual first add-on and can be combined with a moderate statin dose. Other options include bempedoic acid and injectable PCSK9 inhibitors for high-risk cases. Our cholesterol medication guide maps out the full ladder.
The Bottom Line on Atorvastatin vs Rosuvastatin
The atorvastatin vs rosuvastatin debate has a quietly reassuring answer: you are choosing between two genuinely excellent drugs, and the gap between them is far smaller than the gap between taking one and taking nothing. Rosuvastatin lowers LDL further per milligram. Atorvastatin has the longer record and the simpler interaction story. Over three years of head-to-head follow-up, both protected hearts equally well.
So stop optimising the molecule and start optimising the two things that genuinely move your risk: getting to the right intensity, and staying on it.
One thing to do this week: find your last LDL result and the dose you are on, then check them against the intensity table above. If you are on a moderate dose but need a high-intensity drop, that gap — not the brand on the box — is what to raise at your next appointment. Both molecules are available as low-cost generics from WHO-GMP-certified manufacturers in the heart and blood pressure range, so cost should not be what decides your intensity.
Still weighing your options?
- Wondering how statins stack up against everything else that lowers cholesterol? Read our guide to the best cholesterol medications.
- Tried both and tolerated neither? See where pitavastatin fits as an alternative.
Sources and further reading
- Atorvastatin — MedlinePlus (US National Library of Medicine)
- Rosuvastatin — MedlinePlus (US National Library of Medicine)
- Rosuvastatin — NHS
- Grundy et al., 2018 AHA/ACC Guideline on the Management of Blood Cholesterol, Circulation
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.