







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Most people store their medicines in the two worst rooms in the house: the bathroom cabinet and the kitchen windowsill. Both run hot and humid — the exact conditions that quietly drain a drug’s strength. Yet learning how to store medications in hot weather rarely makes it onto anyone’s summer checklist, right up until a heat wave, a hot car, or a scorching mailbox forces the question.
Here’s the reassuring part: heat damage follows rules, and once you know them, protecting your medicine is mostly common sense plus a few non-obvious catches. This guide gives you the plain-English chemistry of why heat degrades drugs, a medicine-by-medicine storage table, a two-minute “was it ruined?” triage, the truth about parked cars, and a travel section from carry-on to hotel room.
One warning up front, and we’ll come back to it: the most dangerous heat damage is the kind you can’t see, taste, or smell. Insulin can look perfectly clear and still have lost much of its punch.
Key Takeaways
- “Room temperature” is a defined range (20–25°C) — but it legally allows brief trips to 30°C, and knowing that one distinction changes everything.
- Heat attacks by two routes: it wrecks biologic drugs (insulin, pens) and pill-based drugs by different chemical mechanisms — so the storage rules differ.
- A parked car runs hotter than you think — summer cabin temperatures climb far past every “room temperature” allowance.
- Some medicines must never go in the fridge — putting one common emergency device in there can make it fail when you need it most.
- There’s a simple triage for “is my medicine still safe?” — and one drug type where you should never guess.
On this page
Why Heat Ruins Medicine (the Two-Minute Chemistry)
Heat speeds up the chemical reactions that break a drug down, so a medicine kept too warm slowly loses potency — and sometimes safety — long before its printed expiry date. That’s the short version. Now the useful detail.
Medicines fall into two camps, and heat attacks each differently.
Biologic drugs — insulin, GLP-1 pens, and many injectables — are built from large, folded proteins. Their shape is their function, like a key cut to a specific lock. Add heat and the protein starts to unfold, or denature. Think of an egg white turning from clear to solid in a hot pan — that change doesn’t reverse on cooling, and a denatured molecule can’t do its job even if the liquid looks fine.
Small-molecule drugs — most tablets, capsules, and many liquids — degrade by other reactions, mainly oxidation (reacting with oxygen) and hydrolysis (breaking apart in water). Heat and humidity accelerate both. That’s why the bathroom is such a poor choice: every hot shower bathes your pills in warm, moist air.
Here’s where it gets interesting. As a rough rule, reaction rates roughly double for every 10°C rise in temperature. So a drug at 40°C isn’t “a little” worse off than one at 20°C — it can degrade several times faster. That’s the invisible cost of a hot glovebox or a sunny windowsill.
Research Spotlight
Drug-stability research consistently shows that potency loss from heat is often invisible. A vial can look, smell, and pour the same while its active ingredient has quietly fallen below the level that makes it work — which is why “it looks fine, so it’s fine” fails for heat-exposed medicine.
The takeaway: you cannot judge heat damage by appearance alone — the chemistry runs silently.
What “Room Temperature” on the Label Really Means
If a leaflet says “store at room temperature,” it isn’t being vague. Behind that phrase sits a formal standard called controlled room temperature.
Under the United States Pharmacopeia definition, controlled room temperature means a range of 20–25°C (68–77°F). Crucially, it also allows for real life: brief excursions between 15°C and 30°C (59–86°F) are permitted, and even short spikes up to 40°C for no more than 24 hours may be tolerated — provided the average thermal exposure over time (the mean kinetic temperature) stays at or below 25°C.
The NHS Specialist Pharmacy Service describes a similar ambient window, noting that ideal storage sits between roughly 15°C and 25°C, while some products are labelled for anywhere from 8°C to 30°C depending on their chemistry. You can read the NHS guidance on ambient storage for the pharmacy-side detail.
So what does this allow? A medicine that briefly reaches 28–30°C on a warm afternoon is usually within tolerance — short excursions are built into the standard. What the standard does not forgive is sustained heat, or the far higher temperatures of a car, attic, or sun-facing windowsill, where readings blow past 40°C and stay there.
In plain terms: the label’s “room temperature” is a budget, not a single number. A quick, mild overshoot spends a little of it. Hours at 50°C in a parked car blows the whole account. This distinction is the heart of room temperature medication storage, and it’s exactly what shallow “keep it cool” advice never explains.
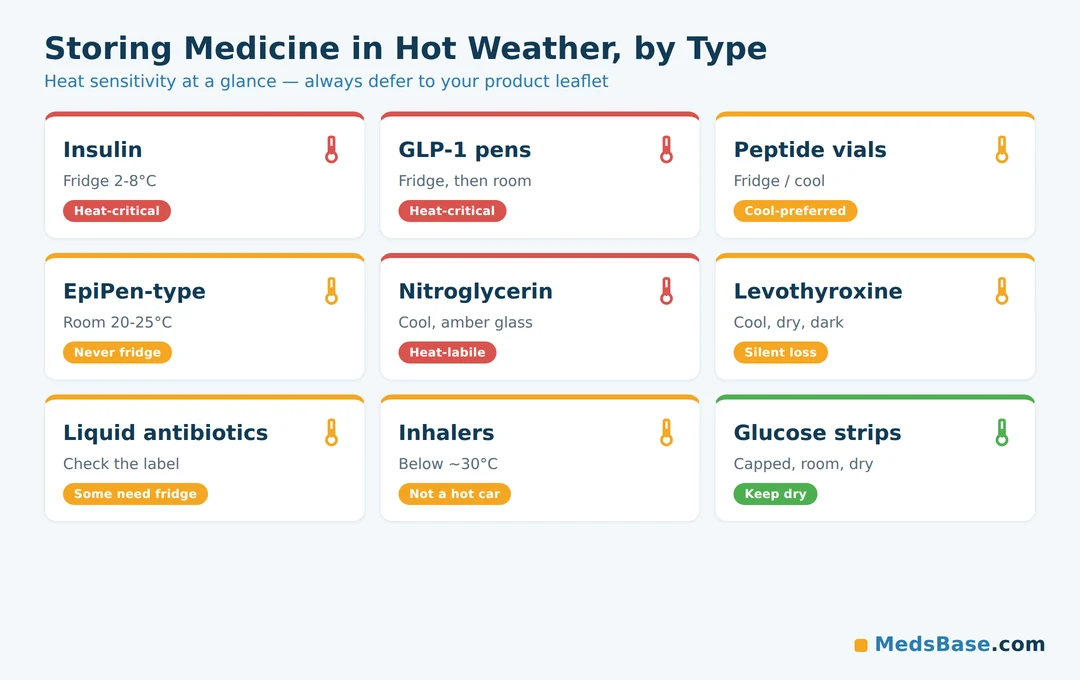
How to Store Medications in Hot Weather, by Type
Different medicines have very different heat tolerances. This table is your field reference. Always defer to your specific product’s leaflet and your pharmacist — formulations vary, and the storage line on your own box wins over any general chart.
| Medication / class | Normal storage | Heat danger zone | Signs it may be compromised | What to do |
|---|---|---|---|---|
| Insulin (unopened) | Fridge 2–8°C (36–46°F) | Above ~30°C, or freezing | Clumps, frosting, clouding of a normally clear insulin, discolouration | Don’t use if you suspect damage; per FDA guidance, vials/cartridges can sit at 15–30°C up to 28 days if needed — confirm with pharmacist |
| Insulin (in-use) | Per label, often ≤25–30°C for a set number of days | Sustained heat above label limit | As above; unexplained loss of blood-sugar control | Track your in-use days; replace if over-limit or heat-exposed; ask pharmacist |
| GLP-1 pens (semaglutide/tirzepatide-type) | Fridge before first use; then per label at room temp for a set window | Heat above label limit; freezing | Cloudiness, particles, damaged pen | Follow the exact in-use day count on your leaflet |
| Peptides — lyophilized (freeze-dried) | Often fridge/freezer per supplier; dry powder is more heat-tolerant | Prolonged warmth; humidity once opened | Discolouration, failure to dissolve cleanly | See our peptide cold-chain deep-dive |
| Peptides — reconstituted (mixed) | Fridge; short shelf life | Any warmth shortens life fast | Cloudiness, particles, colour change | See how long reconstituted solutions last |
| Liquid antibiotics (suspensions) | Varies — some need refrigeration, some do not | Heat degrades many; some separate | Change in colour, smell, or thickness; won’t re-suspend | Check the pharmacy label and ask your pharmacist |
| Levothyroxine (thyroid) | Room temp, protect from heat/light/moisture | Sustained heat can reduce potency | No visible sign — potency loss is silent | Store cool and dry; replace if heat-exposed and ask pharmacist |
| Nitroglycerin (angina) | Original amber glass, cool, tightly closed | Notoriously heat- and light-labile | Tablets that no longer tingle under the tongue may be weak | Keep in original container; don’t decant into pill organisers |
| Epinephrine auto-injector (EpiPen-type) | Room temp ~20–25°C; do NOT refrigerate | Heat degrades epinephrine; so does cold/freezing | Solution discoloured (pink/brown) or containing particles | Never fridge it; replace if discoloured; carry insulated in summer |
| Inhalers (pressurised) | Room temp, below ~30°C | Hot cars — pressurised canister + heat | Reduced spray, damaged canister | Keep out of hot cars; never puncture or incinerate |
| Glucose test strips | Original vial, room temp, dry | Heat and humidity skew readings | Erratic or implausible readings | Keep capped in the original vial; don’t leave in a car |
Notice the two most dangerous surprises: insulin can lose potency with no visible change, and the epinephrine auto-injector must never go in the fridge — a mistake that can weaken an emergency device when it matters most.
Who Is This For? (and Who Should Not Rely on General Advice)
This guide is for anyone managing their own or a family member’s medicines through hot weather. It is not a substitute for your product leaflet or pharmacist — especially if you use insulin, an epinephrine auto-injector, or nitroglycerin, where a wrong call is high-stakes. If you have any of these, treat the pharmacist as your tiebreaker, not this article.
If you manage diabetes, insulin and GLP-1 storage in summer deserves special care — you can browse options and formats across our diabetes medication range and match the storage line to your routine.
A quick word on peptides, because heat tolerance depends on format. A lyophilized (freeze-dried) vial is a dry powder, and dry powders are chemically far more stable against warmth than solutions — a general storage fact worth knowing once a vial is in your hands. Reconstituted (mixed) solutions are the opposite: fragile and short-lived. Research-grade tirzepatide vials are supplied lyophilized for this reason. (Research-grade only; not a claim of approval or a prescribing recommendation.)
“Was It Ruined?” — the Triage That Stops a Guessing Game
You’ve found the meds that sat in a hot car or a scorching mailbox. Now what? Run this triage — it resolves the intro’s open loop (heat damage is often invisible) by giving you a decision path instead of a guess.
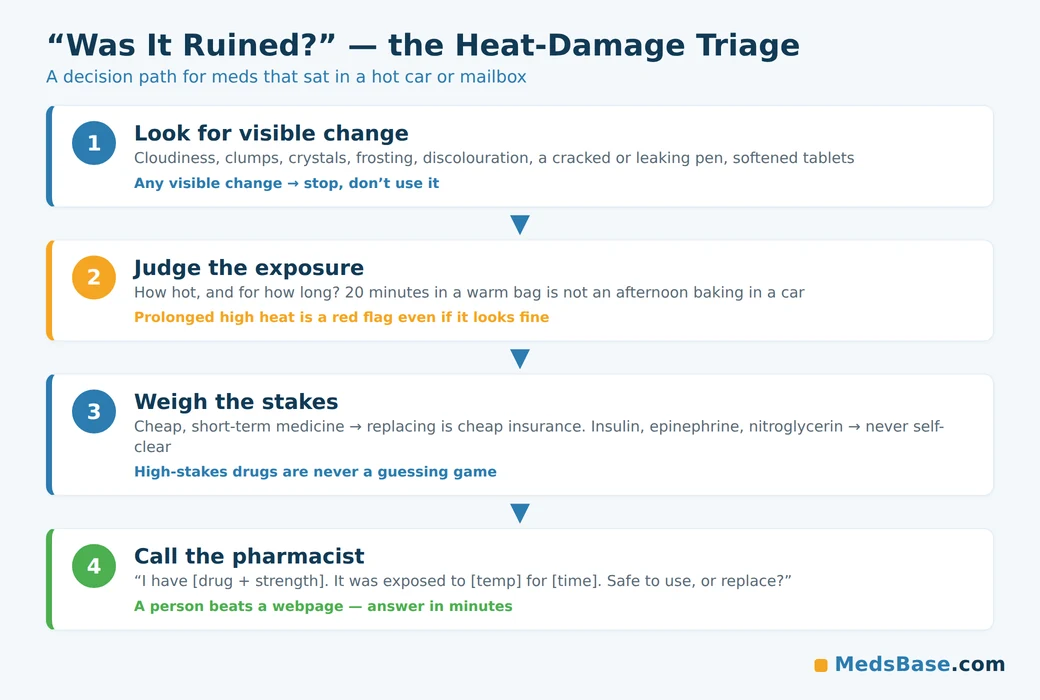
Step 1 — Look for visible changes. Cloudiness in a clear liquid, clumps, crystals, frosting, discolouration, a cracked or leaking pen, tablets that have softened or stuck together. Any visible change is a stop sign — don’t use it, and check with your pharmacist.
Step 2 — Judge the exposure, not just the look. No visible change doesn’t guarantee safety. Ask: how hot, and for how long? A medicine that spent 20 minutes in a warm bag is very different from one that baked in a car all afternoon. Brief, mild excursions are usually within tolerance; prolonged high heat is not.
Step 3 — Weigh the stakes. For a low-risk, inexpensive medicine you use short-term, replacing it after a bad exposure is cheap insurance. For insulin, epinephrine, nitroglycerin, or any medicine you depend on daily, don’t self-clear it. The MedlinePlus guide to storing your medicines is a good reference, but a person beats a webpage here.
Step 4 — Call the pharmacist with a script. You don’t need the chemistry. Say:
“I have [drug name and strength]. It was exposed to about [temperature/situation] for roughly [time]. Is it still safe to use, or should I replace it?”
A pharmacist can check the product’s stability data and answer in minutes. For expensive medicine, the manufacturer’s helpline is a second option — many keep excursion-tolerance data on hand.
Two firm rules keep this safe: never keep using a medicine that looks visibly compromised, and never throw out expensive medicine on a guess — get the pharmacist or manufacturer to confirm first.
The Hot-Car Reality Check (Higher Than You Think)
If you take one habit from this article, make it this: never store medication in a parked car. People underestimate car interiors badly.

Peer-reviewed measurements of parked-car cabins found maximum interior temperatures of 41°C to 76°C (106°F to 169°F), with clear summer days averaging around 68°C inside — hot enough to blow past every “room temperature” allowance many times over. See the parked-car cabin temperature study for the full range.
The catches that trip people up:
- The glovebox is not cooler. It’s an enclosed compartment inside an already-hot cabin — often no better, sometimes worse.
- “Can medications be left in a hot car” for a quick errand? A short stop on a mild day may be fine for a hardy tablet, but there’s no safe window for insulin, pens, or an epinephrine device — and cabin heat builds fast even when the air outside feels tolerable.
- The mailbox and doorstep count too. A metal mailbox in direct sun behaves like a small oven. If a temperature-sensitive medicine is sitting there, bring it indoors promptly and inspect it — check the product on arrival and follow the pharmacist’s guidance if anything looks off.
The simple rule: your car is the one place a medicine should never live in summer, even briefly. Take it with you.
Travelling in Summer: Keeping Meds Safe on the Move
Summer travel adds two heat traps most people miss. Handle these and you’ve covered most of the risk.
Fly carry-on, never checked luggage. Aircraft cargo holds are not reliably climate-controlled and can swing to extremes. Your carry-on stays in the regulated cabin with you, where you can watch the cold packs. This matters most for insulin, pens, and any refrigerated medicine. Keep everything in its original, labelled packaging — it speeds security checks and, per NHS and MedlinePlus guidance, prevents dangerous mix-ups.
Plan the “last mile.” The risky moments are the gaps — the walk across a sun-baked car park, the hour the bag sits in a hire car, the afternoon on a beach. Bridge them with a cool pack or insulated pouch, and get temperature-sensitive medicine into a hotel fridge when you arrive.
A few practical habits for travel medication storage:
- Bring more than you need. A buffer supply covers delays and lets you discard anything you suspect was heat-exposed without running short.
- Avoid the freeze mistake. Cold packs can freeze insulin and epinephrine, which damages them just as heat does. Keep a spacer between the medicine and any frozen gel pack — never let them touch.
- Mind the hotel minibar. Minibar fridges run warm and cycle unevenly; they’re a backup, not a guarantee. Ask the front desk for a proper fridge if you rely on refrigerated medicine.
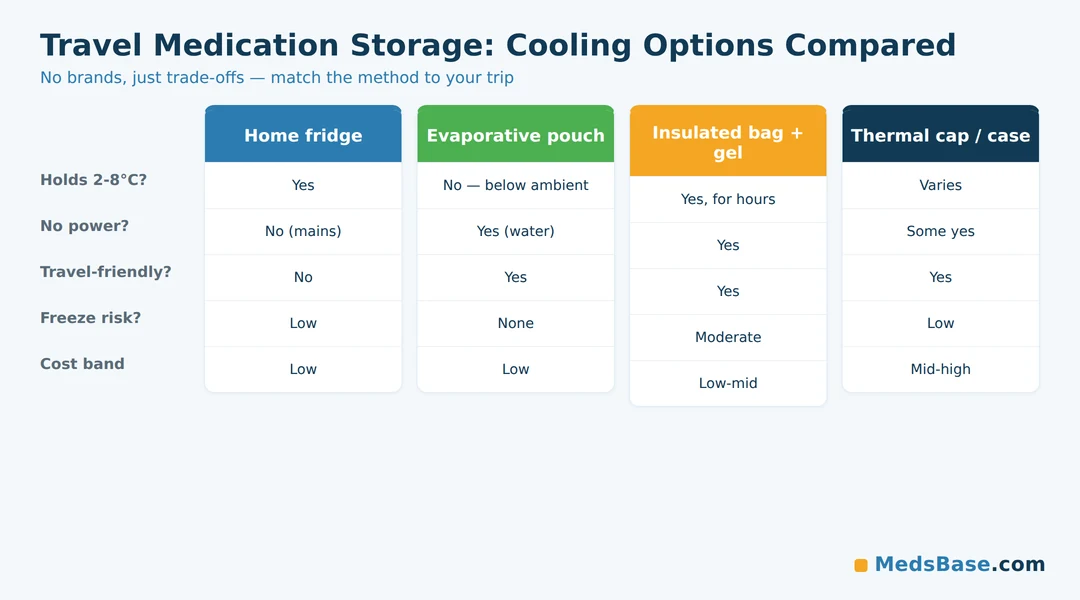
Cooling Options Compared — No Brands, Just Trade-Offs
When “keep it in the fridge” isn’t possible, you have four broad options. Here’s how they compare — generically, with no product or retailer endorsements. Pick by situation, not by marketing.
| Option | Holds 2–8°C? | No power needed? | Travel-friendly? | Freeze risk? | Cost band |
|---|---|---|---|---|---|
| Home fridge | Yes | No (mains) | No | Low (mid-shelf) | Low (owned) |
| Evaporative cooling pouch | No — cools below ambient, not to fridge temps | Yes (needs water) | Yes | None | Low |
| Insulated bag + gel pack | Yes, for hours | Yes | Yes | Moderate — gel can freeze meds | Low–mid |
| Thermal medication cap/case | Varies by design | Some yes | Yes | Low | Mid–high |
Which one fits which situation?
- At home during a heat wave: the fridge, using the middle shelf and keeping medicine off the freezing back wall.
- A day out or commute: an evaporative cooling pouch is light, needs only water, and holds things below the surrounding air — ideal for medicines that need “cool,” not “cold.”
- A longer trip with refrigerated medicine (insulin, pens): an insulated bag with a gel pack holds fridge-range temperatures for hours — just prevent direct contact so nothing freezes.
- All-day carry of a single pen or device: a thermal cap or case is most convenient, at a higher price.
The honest verdict: there is no single “best” cooler — the right choice matches how cold your medicine needs to be and how long you’re away from a fridge. For anything that must stay strictly 2–8°C, an evaporative pouch alone isn’t enough.
What the Research Says
The evidence base for heat and medicine is clear on one point: some drugs tolerate heat well, and others degrade toward failure — and you can’t tell which from the outside.
| Study / source | Year | Finding | Source |
|---|---|---|---|
| Parked-car cabin temperature study | 2009 | Interior maxima ranged 41–76°C; clear summer days averaged ~68°C inside | PubMed |
| Field drug-stability study (heat/cold arms) | 2017 | Morphine and ondansetron stayed >90% potency; atropine became undetectable after 4 weeks of heat; naloxone degraded with heat | PubMed |
| FDA insulin storage guidance | Current | Insulin vials/cartridges can be kept at 15–30°C for up to 28 days if refrigeration is unavailable | FDA |
What this means for you: research confirms the pattern this whole guide is built on — heat damage is real, drug-specific, and largely invisible. A medicine that stays strong in one study can sit beside another that heat destroys, so “it was fine last summer” tells you nothing about this medicine. When in doubt, the label limit and the pharmacist are your evidence base, not the drug’s appearance.
Research here is also honest about its limits: much stability testing covers only a handful of drugs, so exact numbers for your product may not exist publicly. Where data is thin, the safe move is to follow the label and ask a professional — admitting that uncertainty is itself the responsible answer.
How to Store Medications in Hot Weather: a 5-Step Routine
Here’s the practical playbook. Five steps, and you’ve closed the main gaps.
- Move your medicines out of the bathroom and off the kitchen windowsill. Pick a cool, dry, dark spot — a bedroom drawer or a high cupboard away from the oven, radiator, and sun. This one change fixes the most common mistake.
- Read the storage line on every leaflet once. Sort your medicines into three piles: fridge (2–8°C), room temperature (with the excursion allowance you now understand), and “do not refrigerate” (like epinephrine devices).
- Never leave medicine in a parked car — not the glovebox, not the boot, not “just for ten minutes” for anything temperature-sensitive.
- Build a travel kit: original packaging, an insulated bag with a spaced (not touching) cold pack, a buffer supply, and your med list.
- When in doubt, inspect and call. Visible change means stop. Uncertain exposure means phone the pharmacist with the script above.
Common mistakes to avoid:
- Decanting pills into a daily organiser left on a sunny counter (light + heat + no original protection).
- Letting a frozen gel pack touch insulin or an epinephrine device — freezing damages both.
- Assuming colder is always better; the freezing back wall of a fridge can damage medicine too.
Managing insulin or a GLP-1 medicine through summer is the highest-stakes version of all this — it’s worth matching your exact product’s storage window to your daily routine, and you can review formats across our diabetes medication range if you’re comparing options.
Related Reading
- Our peptide cold-chain storage deep-dive — the detailed, peptide-specific companion to this umbrella guide.
- How long reconstituted solutions actually last — shelf life once a vial is mixed.
- The correct way to reconstitute a vial — avoid wasting product to technique errors.
Frequently Asked Questions
Can medications be left in a hot car?
No — not safely for anything temperature-sensitive. Parked-car interiors can reach 41–76°C in summer, far above the 20–25°C “room temperature” range and its brief 30°C allowance. Even a short stop offers no safe window for insulin, pens, inhalers, or an epinephrine device. Take medicine with you instead.
How do you know if medicine has been damaged by heat?
Start with visible signs — cloudiness in a clear liquid, clumps, crystals, discolouration, softened or stuck tablets, a leaking pen. Any of these means stop and check. But heat damage is often invisible, so also judge the exposure: prolonged high heat is a red flag even when the medicine looks normal. When unsure, ask a pharmacist.
What temperature ruins medication?
There’s no single number, but sustained exposure above 30°C is where many medicines start losing potency, and car-cabin heat of 40–70°C degrades them quickly. “Room temperature” allows 20–25°C with brief trips to 30°C; beyond that, especially for hours, the risk climbs sharply. Always check your product’s label limit.
Does heat make medication less effective?
Yes — heat speeds up the reactions that break drugs down, so heat-exposed medicine can lose strength before its expiry date. Biologic drugs like insulin can denature; tablets can oxidise or hydrolyse. Because reduced potency usually can’t be seen, storage rules and expiry dates matter more than appearance.
Can I still use insulin that got warm?
Maybe, but don’t guess. Per FDA guidance, insulin vials and cartridges can tolerate 15–30°C for up to 28 days if refrigeration is unavailable — but sustained higher heat or freezing can ruin it, sometimes invisibly. Check for clumps, frosting, or clouding, and confirm with your pharmacist before relying on it for blood-sugar control.
What about medicine I received during a summer heat wave?
Focus on what you can control: inspect the medicine as soon as it reaches you, bring it indoors promptly rather than leaving it in a hot mailbox, and check for any visible change. If anything looks off, or you’re unsure whether it was heat-exposed, ask your pharmacist before using it.
How do you keep medication cool while travelling?
Pack it in your carry-on, never checked luggage, since cargo holds aren’t reliably climate-controlled. Use an insulated bag with a cold pack that doesn’t touch the medicine directly (to avoid freezing), keep everything in original packaging, and move refrigerated medicine into a proper fridge as soon as you reach your destination.
Is the bathroom cabinet really a bad place to store medicine?
Yes — it’s one of the worst. Showers create repeated bursts of heat and humidity, and moisture accelerates the breakdown of many tablets. A cool, dry bedroom drawer is a far better default for most room-temperature medicines.
The Bottom Line
Learning how to store medications in hot weather comes down to a few durable habits: keep medicines cool, dry, and out of the bathroom; respect the difference between a brief excursion and hours of real heat; never use a parked car as storage; and treat insulin, epinephrine, and nitroglycerin as high-stakes cases where the pharmacist decides, not your eyes. Heat damage is real but rule-bound — and now you know the rules.
Your one immediate action: tonight, move your medicines out of the bathroom and off any sunny surface, and skim each leaflet’s storage line to sort them into fridge, room-temperature, and never-refrigerate piles. Fifteen minutes now prevents a summer of quiet potency loss.
If you’re managing diabetes or weight medicine through the heat, match your exact product’s storage window to your routine — you can compare formats across our diabetes medication range.
Two natural next questions:
- Worried a heat-weakened pen could throw off your dose? Read our companion guide on semaglutide overdose and dosing mistakes — uncertain potency and dosing errors are two sides of the same risk.
- Wondering which everyday medicines don’t mind the heat? Statins like atorvastatin and rosuvastatin are stable at room temperature (though still not in a 70°C car) — see our atorvastatin vs rosuvastatin comparison for how the two differ where it counts.
Medical Disclaimer
This article is for general information and education only. It is not medical advice and does not replace your medicine’s patient information leaflet or the guidance of your doctor or pharmacist. Storage requirements vary by product and formulation. Never continue using a medicine you believe may be compromised, and never discard costly medicine without first confirming with your pharmacist or the manufacturer’s helpline. For medicines where an error is high-stakes — including insulin, epinephrine auto-injectors, and nitroglycerin — always seek professional confirmation.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.