







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Quick Answer: An oral PCSK9 inhibitor is a daily tablet that lowers LDL (“bad”) cholesterol by blocking PCSK9, a protein that destroys the liver’s LDL-clearing receptors. In July 2026 the FDA approved the first one — enlicitide (brand name Lipfendra) — which cut LDL by about 57% in its main trial, matching results once possible only with injections.

For years, the most powerful cholesterol drugs after statins came with a catch: you had to inject them. That changed on July 16, 2026, when regulators approved the first oral PCSK9 inhibitor — a once-daily pill in a class that had been needles-only since 2015.
By the end of this article, you’ll know exactly how this pill works, how far it drops LDL cholesterol, who stands to benefit most, and — just as importantly — who probably doesn’t need it yet. We’ll also cover one detail about access that most headlines skip, and how today’s proven statins still fit into the picture.
Here’s the part that surprises people: the size of the LDL drop isn’t the only thing that matters. One number buried in the trial data tells you more about your heart risk than the headline percentage does — we’ll get to it in the research section.
Key Takeaways
- ✔ The first oral PCSK9 inhibitor (enlicitide / Lipfendra) won FDA approval on July 16, 2026 — but the class itself isn’t new, only the pill form is.
- ✔ In its main trial it cut LDL cholesterol about 57% — yet a different number predicts heart risk even better.
- ✔ It’s a once-daily tablet, but one common habit can blunt any oral drug’s benefit; we’ll flag it.
- ✔ It’s not a statin replacement for most people — the honest “who should skip this” is in the safety section.
- ✔ Access and cost, not biology, will decide who actually gets it first.
On this page
What Is an Oral PCSK9 Inhibitor?
An oral PCSK9 inhibitor is a swallowed medicine that lowers LDL cholesterol by shutting down PCSK9 — a protein that tells your liver to destroy the very receptors it uses to pull cholesterol out of your blood. Block PCSK9, and those receptors survive longer, clearing more LDL. Enlicitide is the first pill to do this.
Until now, this drug class existed only as injections given every two to four weeks (or twice a year for a related option). They worked well — but needles, refrigeration, and specialty-pharmacy hoops kept many people away. For a person who is already managing a statin, a blood-pressure pill, and a busy life, “and now inject yourself on a schedule” was often the step too far. Cholesterol has no symptoms, so the motivation to keep up an inconvenient treatment is thin — which is precisely why an easier delivery method can translate into better real-world protection.
The new PCSK9 inhibitor pill aims to remove that friction. Same target, same biology, delivered as a tablet you take at home. That shift — from clinic injection to kitchen-counter pill — is why cardiologists have called this one of the more practical cholesterol advances in a decade.
Why does LDL matter so much in the first place? Because it’s the cholesterol that builds plaque in your arteries, and decades of research tie higher LDL to more heart attacks and strokes. The NIH’s cardiovascular resources frame LDL as a core, modifiable risk factor — meaning the lower you drive it (within reason and under guidance), the more you cut that risk. That’s the whole rationale behind a drug this powerful: for the right person, a bigger LDL drop can mean a meaningfully lower chance of a cardiac event down the road.
To understand why that matters, it helps to know where PCSK9 inhibitors sit in the cholesterol toolkit. Statins came first and remain the foundation. Ezetimibe, a gentle add-on, blocks cholesterol absorption in the gut. Injectable PCSK9 inhibitors arrived in 2015 as the heavy artillery — reserved for people who needed a big LDL drop that statins alone couldn’t deliver. They were effective, but the practical barriers were real: many patients never filled the prescription, and among those who did, a meaningful share stopped within a year. An oral PCSK9 inhibitor attacks that adherence problem directly, because a pill is simply easier to keep taking than a scheduled injection.
There’s a second reason the pill matters: reach. Injectables largely stayed inside cardiology clinics and specialty pharmacies. A tablet can be prescribed and refilled through ordinary channels, which means far more people who need aggressive LDL lowering could realistically get it. Biology sets the ceiling on how well a drug works; convenience decides how many people benefit in the real world.
In one line: it’s the injection’s power in a pill you can actually stick with.
How Does an Oral PCSK9 Inhibitor Work?
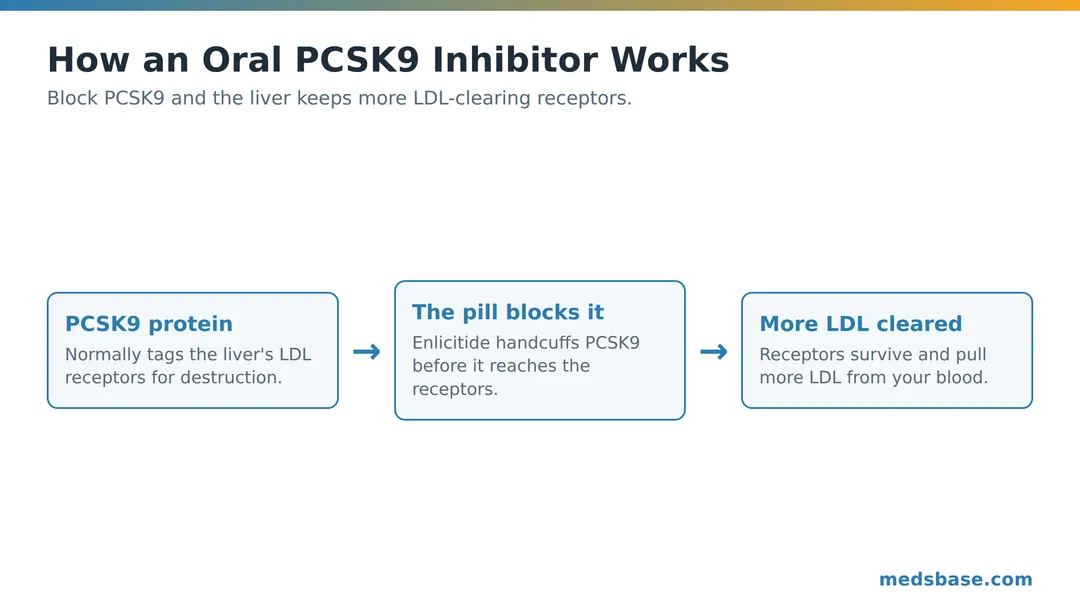
Picture your liver as a recycling plant with thousands of little claw machines on its surface — LDL receptors. Each claw grabs an LDL particle from your bloodstream and pulls it in for disposal. The more claws you have, the lower your LDL.
PCSK9 is the saboteur. It latches onto those claws and drags them to the shredder, so the liver has to keep building new ones. People with naturally high PCSK9 have fewer working claws and higher LDL. An oral PCSK9 inhibitor handcuffs PCSK9 before it can reach the claws — so the receptors keep working shift after shift.
Research Spotlight: PCSK9 was discovered through families with sky-high cholesterol caused by an overactive version of the gene — and others with strikingly low cholesterol and a broken version. That natural experiment, catalogued in the NIH genetics database, is exactly why blocking PCSK9 lowers LDL so reliably.
Statins work differently — they slow how much cholesterol your liver makes, which prompts it to build more receptors too. That’s why the two approaches stack so well: statins raise receptor demand, and a PCSK9 inhibitor stops those receptors being destroyed. Different levers, same goal — a lower LDL number.
Take Sarah, 52 (an illustrative example, not a real patient). She’s on the highest statin dose she can tolerate, exercises, eats carefully — and her LDL still sits stubbornly above target because her body runs high on PCSK9. Adding an oral PCSK9 inhibitor wouldn’t replace her statin; it would stop her hard-won LDL receptors from being shredded, letting the statin she already takes finally do its full job. That combination scenario — statin plus PCSK9 inhibitor — is the most common way these drugs are actually used.
What makes the oral version scientifically clever is the chemistry. PCSK9 is a large protein, and proteins are usually destroyed in the stomach before they can be absorbed — which is exactly why the first PCSK9 inhibitors had to be injected. Enlicitide is engineered as a small, stable molecule that survives digestion well enough to reach the bloodstream in a pill. Solving that “how do you swallow a protein-blocker” puzzle is the real breakthrough here, more than the LDL numbers themselves.
Who an Oral PCSK9 Inhibitor Is For — and Who Can Wait
This is where the hype needs a reality check. A powerful LDL-lowering pill sounds like something everyone with high cholesterol should want. In practice, it’s aimed at specific groups.
People who are still above goal on a statin
If you take the strongest statin dose you can tolerate and your LDL is still higher than your target, adding a PCSK9 inhibitor is a logical next step. This is the largest real-world use.
People who can’t tolerate statins
A minority of patients get genuine muscle symptoms on statins. For them, an oral PCSK9 inhibitor offers strong LDL lowering without the statin.
People with familial hypercholesterolemia
This inherited condition causes very high LDL from birth and often needs more than one drug. PCSK9 inhibitors have become a cornerstone here.
People at high cardiovascular risk who need a bigger drop
After a heart attack or with established artery disease, guidelines push LDL very low — often below 55 mg/dL. Reaching those aggressive targets frequently takes more than a statin, and a PCSK9 inhibitor is one of the most reliable ways to close the gap. In the CORALreef Lipids trial, roughly seven in ten participants hit both a 50%-or-greater LDL cut and an LDL under 70 mg/dL — the kind of dual target that’s hard to reach with older drugs.
People with high lipoprotein(a)
Lp(a) is an inherited, cholesterol-carrying particle that raises heart risk and barely responds to statins or diet. It’s one of the frustrations of preventive cardiology. PCSK9 inhibitors, including this oral one, lower Lp(a) by roughly a quarter — not a cure, but a meaningful move for people who have few other options. If you’ve ever been told your Lp(a) is high, this is a reason to ask your doctor about the class.
Who Is This For? / Who Should Avoid It?
Good fit: high-risk heart patients, statin-intolerant patients, familial hypercholesterolemia, or anyone not at LDL goal on maximal statin therapy.
Should wait or skip: people with mildly elevated LDL who haven’t yet tried a statin and lifestyle changes; anyone whose cholesterol is already at goal; and — for now — anyone for whom cost or access makes a proven, inexpensive statin the smarter first move. Pregnancy and breastfeeding require a doctor’s individualized advice.
For most people reading this, the honest starting point is still a statin. If you’re weighing your options there, our guide to the best cholesterol medications lays out every class in plain language, and MedsBase stocks widely used statins across the High Cholesterol Treatments range.
Oral PCSK9 Inhibitor Safety, Side Effects & Dosing
Here’s the safety open loop resolved: in the main trial, serious side effects were actually a touch less common on the drug than on placebo. That’s reassuring — but “well tolerated” is not “side-effect free,” and long-term outcome data is still maturing.
| Side effect | Frequency | Severity | What to do |
|---|---|---|---|
| Mild stomach upset / nausea | Occasional | Mild | Take consistently; usually settles |
| Muscle aches | Uncommon | Mild–moderate | Report persistent pain to your doctor |
| Cold-like / upper-respiratory symptoms | Occasional | Mild | Symptomatic care; rarely drug-related |
| Injection-site reactions | None (it’s a pill) | — | A key advantage over injectables |
| Serious adverse events | ~10% vs ~12% on placebo | Varies | Same medical follow-up as any heart drug |
Dosing in brief: the approved oral PCSK9 inhibitor is taken once daily. Because absorption of oral peptide-style drugs can be affected by food and timing, follow the label and your pharmacist’s instructions precisely — an inconsistent routine is the fastest way to lose the benefit you’re paying for.
One honest limitation: PCSK9 inhibitors lower LDL impressively, but the pill’s long-term proof that it prevents heart attacks and strokes is still being gathered. The injectables have that outcome evidence; the pill is expected to follow but isn’t there yet. Where the evidence is still maturing, it’s fair to say so.
A quick word on drug interactions and monitoring. Unlike statins, PCSK9 inhibitors don’t rely heavily on the liver enzyme pathways that cause many cholesterol-drug interactions, which is part of why they combine cleanly with statins. Still, your clinician will likely check a lipid panel a few weeks after you start, and periodically after that. There’s no need for the intensive muscle-enzyme or liver monitoring some people associate with statins, but “low-maintenance” is not “no-maintenance” — a follow-up blood test is how you confirm the drug is doing what it should.
Pharmacists see one predictable mistake with any strong LDL-lowering drug: patients feel completely normal — because high cholesterol has no symptoms — and quietly let the prescription lapse. With PCSK9 inhibitors, LDL climbs back within weeks of stopping. The medicine only works while you’re taking it, and the absence of symptoms is not a sign you’ve been cured.
What Does the Research Say?
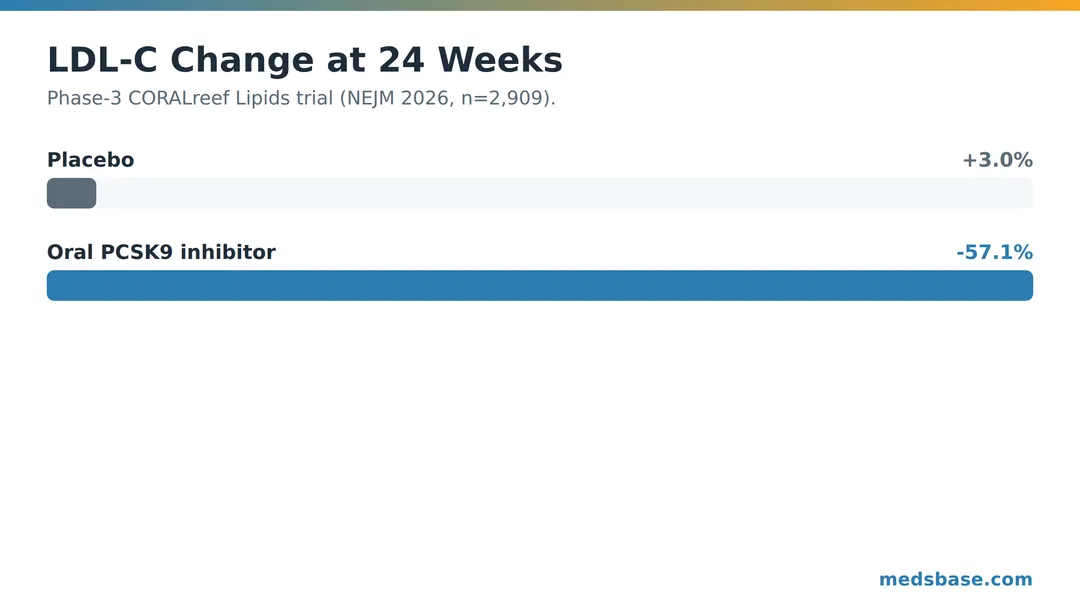
The approval rests largely on a phase-3 trial called CORALreef Lipids, published in the New England Journal of Medicine.
| Study | Year | Finding | Source |
|---|---|---|---|
| CORALreef Lipids (NEJM) | 2026 | LDL −57.1% vs +3.0% on placebo at 24 weeks (2,909 patients) | PMID 41879224 |
| CORALreef Lipids — goal attainment | 2026 | ~70% reached both ≥50% LDL cut and LDL <70 mg/dL | PMID 41879224 |
| CORALreef Lipids — other lipids | 2026 | ApoB −50%, non-HDL −53%, Lp(a) −28% | ACC journal scan |
Now that number we teased. The headline is “57% LDL reduction,” but cardiologists often watch ApoB — a count of the actual atherogenic particles — and it fell about 50%. LDL tells you the cholesterol carried; ApoB tells you how many dangerous particles are doing the carrying, which many researchers consider the truer risk signal.
The enlicitide program didn’t stop at one trial. Separate CORALreef studies tested the drug in people with familial hypercholesterolemia and as an add-on for patients already on statins who still hadn’t reached goal — and in both, it produced the same large LDL reductions. That consistency across different patient types is part of why regulators moved to approval: the effect wasn’t a fluke of one carefully chosen population.
It’s worth putting the 57% figure in context. A moderate statin lowers LDL around 30%; a high-intensity statin, up to about 50%. So an oral PCSK9 inhibitor roughly matches or exceeds a maximal statin — but on top of one, the drops stack, which is how patients reach those very low targets. The trial also reported that adverse events were similar between drug and placebo, which is unusual for a medicine this potent and a genuine point in its favor.
What this means for you: the research suggests an oral PCSK9 inhibitor can drive LDL down as far as injections did — a genuine milestone. What it does not yet prove is a matching drop in heart attacks from the pill specifically; that outcome evidence is still being collected in longer trials, so early enthusiasm should stay measured. Lower LDL strongly predicts fewer heart events across decades of research, but “strongly predicts” is not the same as “proven for this exact pill” — and a good clinician will make that distinction with you.
Oral PCSK9 Inhibitor vs Statins vs Injections
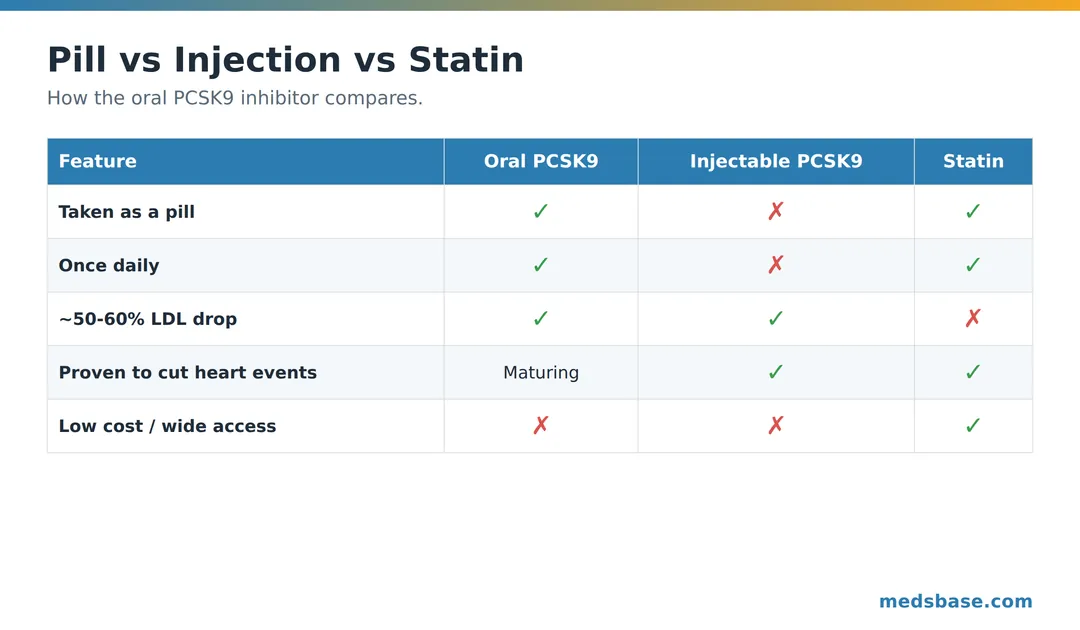
| Feature | Oral PCSK9 inhibitor | Injectable PCSK9 inhibitor | Statin |
|---|---|---|---|
| Route | Pill | Injection | Pill |
| Frequency | Once daily | Every 2–4 weeks (or 2×/yr) | Once daily |
| Typical LDL drop | ~50–60% | ~50–60% | ~30–50% |
| Proven to cut heart events | Maturing | Yes | Yes (decades) |
| Cost / access | Newest, likely priciest at launch | High, specialty | Low, widely available |
Which fits which situation? If you’re doing well on a statin and at goal, you likely need nothing new. If you’re not at goal or can’t take statins, a PCSK9 inhibitor is the add-on — and now the choice between pill and injection can come down to your preference. Some people will still prefer an every-two-weeks injection precisely because they don’t want a daily pill to remember; others will find a tablet far easier to live with. Neither is wrong. But for sheer proven, affordable protection today, the statin remains the backbone. Our head-to-head on atorvastatin vs rosuvastatin is the natural next read if a statin is where you actually are.
There’s also a cost dimension the comparison table can’t capture. Statins are among the least expensive prescriptions in modern medicine — often a few dollars a month as generics. A brand-new oral PCSK9 inhibitor will launch at a premium, and insurance coverage for a just-approved drug typically lags behind approval by months, sometimes with step-therapy requirements that ask you to fail cheaper options first. For a lot of people, the practical answer in 2026 will be: optimize the statin, add ezetimibe if needed, and reserve the PCSK9 inhibitor for when those aren’t enough. That’s not a knock on the new drug — it’s how cost-effective, evidence-based prescribing works.
How to Use an Oral PCSK9 Inhibitor — Practical Guidance
- Confirm you’re the right candidate. This is an add-on or statin-alternative decision made with your clinician, not a first-line self-start.
- Take it once daily, consistently. Same time each day; follow the label’s food instructions exactly.
- Keep your statin unless told otherwise. For most people the two work together, not instead of each other.
- Recheck lipids in 4–12 weeks. The drop is fast; a follow-up panel confirms you’ve hit target.
- Don’t stop on your own. LDL rebounds when you quit — as with any cholesterol drug, stopping undoes the benefit.
Mistakes to avoid: skipping doses because “cholesterol has no symptoms”; assuming the pill lets you drop lifestyle changes; and expecting insurance to cover a brand-new drug instantly. While that access sorts itself out, browse proven statin options in the High Cholesterol Treatments range at MedsBase.
Related reading
Frequently Asked Questions
What is an oral PCSK9 inhibitor?
It’s a daily pill that lowers LDL cholesterol by blocking PCSK9, a protein that destroys the liver’s LDL-clearing receptors. The first one, enlicitide (Lipfendra), was FDA-approved in July 2026 — earlier drugs in this class were injections only.
How does enlicitide lower cholesterol?
It stops PCSK9 from degrading LDL receptors on liver cells. With more receptors surviving, the liver removes more LDL from your blood. In its main trial, this cut LDL about 57%.
Is an oral PCSK9 inhibitor better than a statin?
It lowers LDL more on average, but “better” depends on you. Statins have decades of proof that they prevent heart attacks and are inexpensive. A PCSK9 inhibitor is usually added when a statin alone isn’t enough, or used when statins aren’t tolerated.
Who should take an oral PCSK9 inhibitor?
Mainly high-risk heart patients not at LDL goal on maximal statins, people who can’t tolerate statins, and those with familial hypercholesterolemia. People with mild, untreated high cholesterol should generally try a statin and lifestyle changes first.
Are PCSK9 inhibitor pills safe?
In trials the oral PCSK9 inhibitor was well tolerated, with serious side effects no more common than placebo. Long-term data on preventing heart attacks from the pill specifically is still being gathered, so ongoing doctor follow-up matters.
Will I still need my statin?
Usually yes. For most people the two are combined, not swapped — statins raise LDL-receptor demand while the PCSK9 inhibitor stops those receptors being destroyed. The exception is patients who genuinely can’t tolerate statins, who may use the PCSK9 inhibitor on its own.
How much does an oral PCSK9 inhibitor cost?
As a newly approved brand-name drug, it will be considerably more expensive than generic statins, and insurance coverage often takes months to settle after approval. Many patients will need to try lower-cost options first. Ask your pharmacist about coverage and any manufacturer support programs before assuming the price.
Can an oral PCSK9 inhibitor replace a healthy lifestyle?
No. Diet, physical activity, not smoking, and weight management still shape your heart risk independently of your LDL number. Medication lowers one important risk factor; it doesn’t undo the others. The best results come from combining the two.
The Bottom Line
The arrival of the first oral PCSK9 inhibitor is a real milestone: injection-level LDL lowering, now in a once-daily pill. For high-risk patients who can’t reach their target — or can’t take statins — it’s a genuinely useful new tool, and removing the needle will help people actually stay on treatment.
But temper the excitement with two facts: the pill’s proof that it prevents heart attacks (not just lowers LDL) is still maturing, and for most people a proven, affordable statin is still the right first move. Your immediate action: if you don’t know your current LDL, get a lipid panel — you can’t judge whether you need a powerful add-on until you know your number.
Wondering whether a statin alone is enough for you? Read atorvastatin vs rosuvastatin. Managing blood pressure alongside cholesterol? See our telmisartan vs losartan breakdown next.
Medical Disclaimer
This article is for general education and is not medical advice. Cholesterol treatment decisions — including whether to add a PCSK9 inhibitor — should be made with your doctor or pharmacist based on your personal risk. Never start or stop a prescription medicine on your own.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.