







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Quick Answer: In telmisartan vs losartan, both are angiotensin receptor blockers (ARBs) that lower blood pressure by relaxing blood vessels. Telmisartan lasts longer (about a 24-hour half-life) and controls blood pressure more consistently overnight and into the next morning, and it has unique evidence for preventing cardiovascular events. Losartan is well-established, gentle, and may suit people who also need help with uric acid. The best choice depends on your specific needs.
Your doctor mentions switching your blood pressure pill — or you notice two similar-sounding drugs and wonder whether one is genuinely better. If you’re weighing telmisartan vs losartan, you deserve more than “they’re basically the same,” because in a few ways that matter, they aren’t.
By the end of this comparison you’ll know how these two ARBs differ in strength, how long they last, which one has heart-protection evidence the other lacks, how their side effects compare, and — crucially — which situations favor each. This is a decision guide, not a verdict, because the “better” drug is the one that fits you.
Here’s the tension worth resolving up front: telmisartan looks stronger on paper, yet losartan remains one of the most-prescribed ARBs in the world. Both facts are true, and the reason why is the most useful thing in this article.
Key Takeaways
- ✔ In telmisartan vs losartan, telmisartan has the longer half-life — but that advantage matters more for some people than others.
- ✔ One of these two is the only ARB with a specific type of cardiovascular-protection evidence; we’ll name it.
- ✔ Losartan has a quiet bonus effect that can make it the smarter pick for certain patients.
- ✔ Their side-effect profiles are similar — with one practical difference worth knowing.
- ✔ “Stronger” and “better for you” are not the same thing, and the ending explains why.
On this page
What Are Telmisartan and Losartan?
Both telmisartan and losartan are angiotensin receptor blockers (ARBs) — a class of blood pressure medicines that relax your blood vessels so blood flows with less resistance. Losartan, introduced in the 1990s, was the first ARB ever approved. Telmisartan came later and was engineered for a longer duration of action.
They treat the same core conditions: high blood pressure, and in various cases, heart and kidney protection. Because they share a mechanism, they also share the ARB class’s biggest selling point — they’re well tolerated, and unlike the older ACE inhibitors, they rarely cause the nagging dry cough that drives so many people to switch.
So if they’re cousins in the same family, why compare them at all? Because the family resemblance hides real differences in how long each drug works, how consistently it controls blood pressure around the clock, and what each has been proven to do beyond lowering the number on the cuff. That’s where telmisartan vs losartan gets interesting.
It helps to know where ARBs sit among blood-pressure drugs generally. The main classes are ACE inhibitors, ARBs, calcium channel blockers, and diuretics. ACE inhibitors and ARBs both act on the same hormone system (the renin-angiotensin system), which is why they’re often discussed together — but ARBs block the receptor directly, while ACE inhibitors block the enzyme that makes the hormone. The practical upshot for patients is that ARBs like telmisartan and losartan give ACE-inhibitor-level benefits without the dry cough, which is exactly why so many people who can’t tolerate an ACE inhibitor end up on one of these two drugs.
Both are also used beyond blood pressure alone. ARBs help protect the kidneys in people with diabetes, and they’re used in certain heart conditions. So when your doctor picks between telmisartan and losartan, they may be weighing more than your blood pressure reading — your kidneys, your heart history, and your other conditions all feed into the choice.
How ARBs Like Telmisartan and Losartan Work
Your body makes a hormone called angiotensin II that acts like a drawstring on your blood vessels — it tightens them, which raises blood pressure. It also nudges your body to hold onto salt and water, raising pressure further.
ARBs block the receptor that angiotensin II plugs into. Think of it as putting a cap over the keyhole: the hormone is still there, but it can’t turn the lock. The vessels stay relaxed, salt and water balance improves, and blood pressure falls.
Research Spotlight: Both drugs target the same AT1 receptor, but they don’t hold on equally tightly or for equally long. Telmisartan binds firmly and clears from the body slowly, which is the mechanical reason behind its round-the-clock effect — a difference measured directly in head-to-head trials summarized by the NIH’s hypertension resources.
Losartan has a twist: it’s partly converted in the body to an active metabolite that does much of the blood-pressure work and lasts longer than losartan itself. That’s why losartan is usually effective once daily despite the parent drug’s shorter life. Same lock, slightly different keys — and the key’s staying power is the crux of this comparison.
Telmisartan vs Losartan: Head-to-Head
Here’s the comparison at a glance, before we unpack the parts that matter most.
| Feature | Telmisartan | Losartan |
|---|---|---|
| Class | ARB | ARB (first ever approved) |
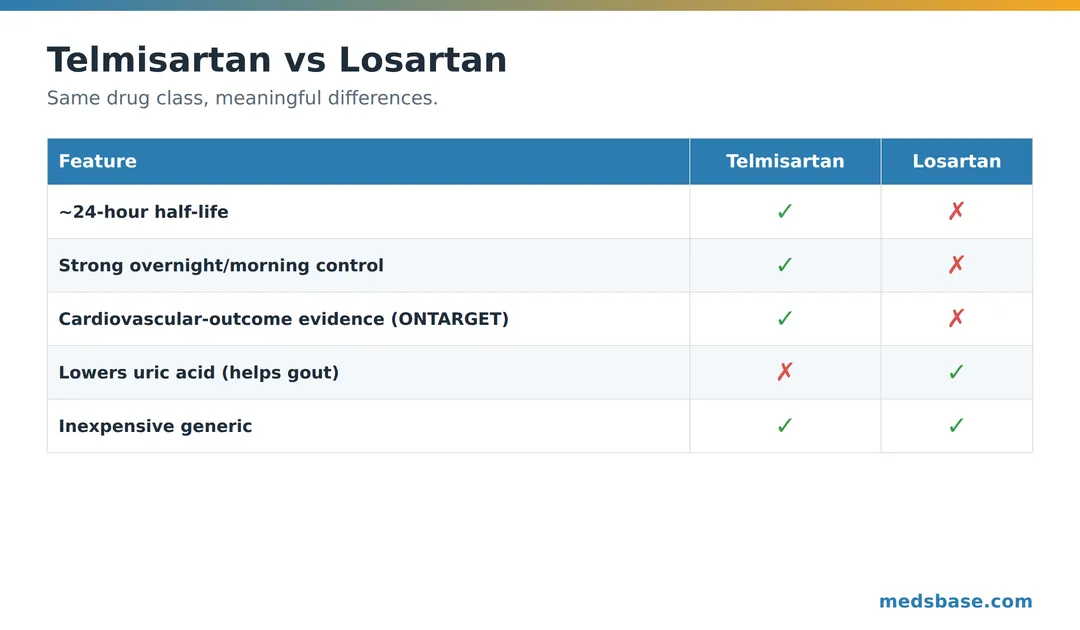
| Half-life | ~24 hours | ~2 h (parent); ~6–9 h (active metabolite) |
| 24-hour BP control | Slightly stronger, esp. overnight/morning | Effective, may fade late in the interval |
| Cardiovascular-outcome evidence | Yes (ONTARGET) | Established in hypertension; different evidence base |
| Bonus effect | Metabolic-neutral, long duration | Lowers uric acid (helpful in gout) |
| Typical dosing | Once daily | Once daily |
| Cost | Inexpensive generic | Inexpensive generic |
Two rows deserve their own sections: the half-life and the cardiovascular evidence. Let’s take them in turn.
The Half-Life Difference That Matters
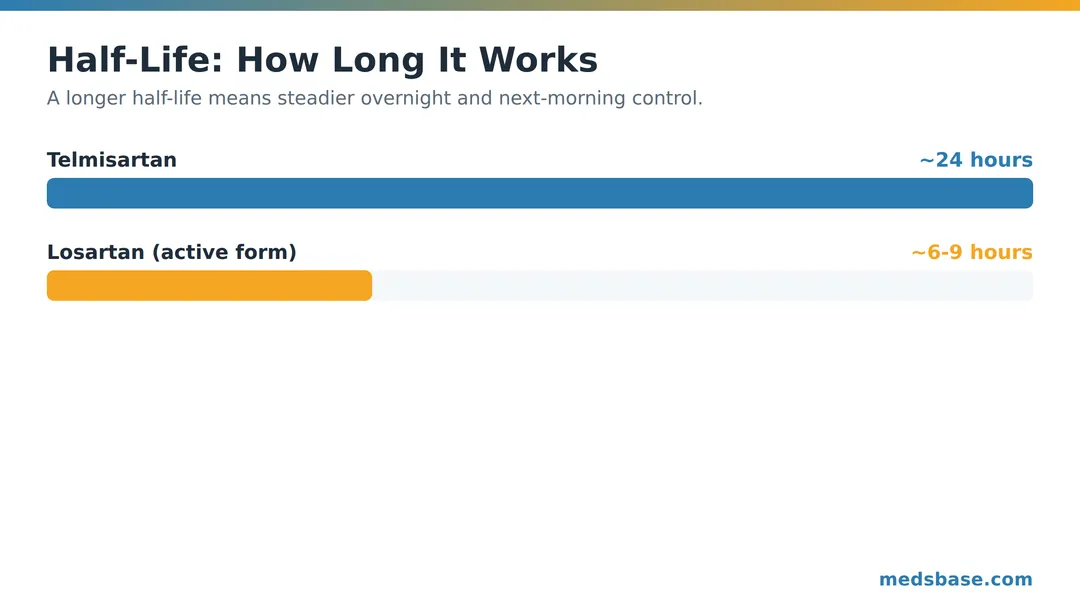
This is the headline advantage for telmisartan. Its half-life is roughly 24 hours — one of the longest of any ARB — while losartan’s parent drug lasts only a couple of hours, relying on its active metabolite (about 6–9 hours) to carry it through the day.
Why does that matter to you? Because blood pressure isn’t only a daytime problem. The hours that predict cardiovascular risk most strongly include the overnight period and the early-morning surge, when heart attacks and strokes cluster. A drug that’s still working strongly at hour 20–24 protects that vulnerable window better.
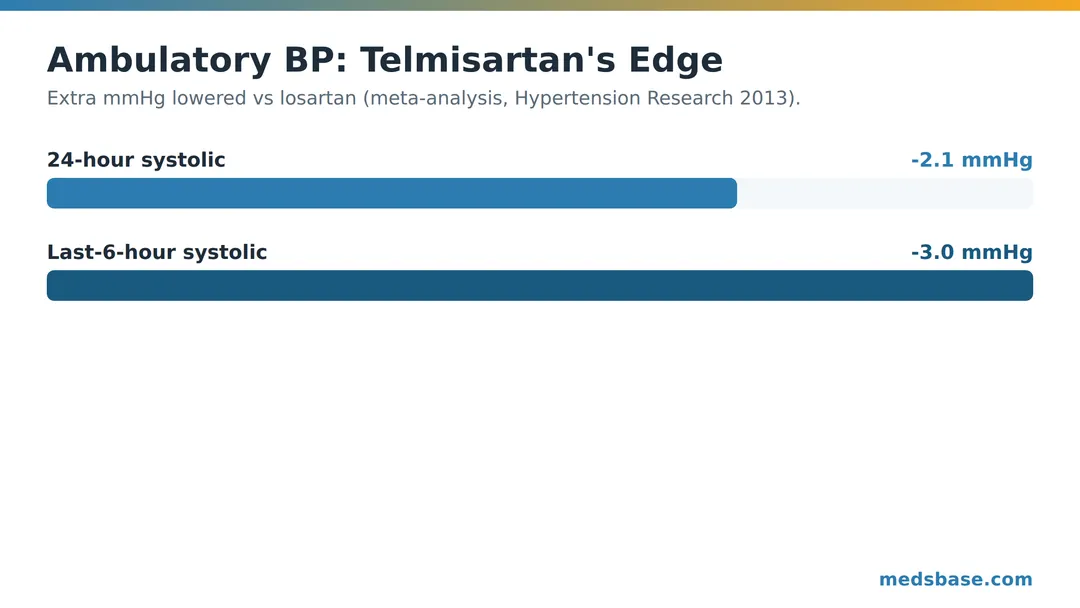
Head-to-head trials bear this out. In a meta-analysis of randomized trials, telmisartan lowered 24-hour ambulatory blood pressure modestly more than losartan — and the gap was largest during the last 6 hours of the dosing interval, exactly the stretch that matters for next-morning protection.
The one-line takeaway: telmisartan’s edge isn’t a bigger daytime drop — it’s a steadier one that doesn’t fade before your next dose.
For most people the difference is modest, a couple of millimeters of mercury. But if your blood pressure runs high in the morning, or you sometimes forget a dose (that long half-life is more forgiving of a late pill), telmisartan’s staying power is a genuine, practical advantage. This is one reason clinicians reach for it, and MedsBase stocks it as Telma.
Consider Priya, 58 (an illustrative example, not a real patient). Her home monitor kept showing high readings first thing in the morning, even though her afternoon numbers looked fine on losartan. That pattern — a fading effect by the end of the dosing interval — is exactly the scenario where a longer-acting ARB earns its keep. Switching to telmisartan smoothed out her mornings, not because it’s a “stronger” drug in some general sense, but because its effect was still going strong when hers had thinned out. The lesson isn’t “telmisartan for everyone” — it’s “match the drug’s duration to your body’s pattern,” which is something a week of home readings can reveal.
A quick note on dosing. Both drugs are taken once daily, with or without food, at whatever time you’ll reliably remember. Telmisartan commonly starts around 40 mg (with room to increase), and losartan around 50 mg (also adjustable), though your doctor sets the exact dose. Because both can lower blood pressure noticeably after the first doses, your clinician may check your readings and a blood test within a few weeks of starting or changing either one.
Cardiovascular Protection: Where They Truly Differ
Here’s the evidence gap we teased. Lowering blood pressure is good, but what patients ultimately care about is fewer heart attacks and strokes. And on that front, telmisartan carries a distinction few ARBs can claim.
In the large ONTARGET trial — over 25,000 high-risk patients followed for years — telmisartan was shown to be non-inferior to ramipril, a gold-standard ACE inhibitor, for preventing cardiovascular events like heart attack, stroke, and cardiovascular death. Crucially, telmisartan achieved that with less cough and less angioedema than the ACE inhibitor. That makes telmisartan one of the few ARBs with direct, high-quality evidence for cardiovascular protection in a broad high-risk population.
Losartan is far from unproven — it has its own strong evidence base in hypertension and in specific groups (notably patients with left ventricular hypertrophy and certain kidney conditions). But it doesn’t carry the same broad, ramipril-equivalent cardiovascular-outcome credential that telmisartan earned in ONTARGET.
What this means for you: if you’re a higher-risk patient — established heart disease, diabetes with organ involvement — that ONTARGET evidence is a real point in telmisartan’s favor. If you’re managing straightforward high blood pressure, both drugs lower it effectively, and the choice hinges more on the other factors below.
The metabolic angle for people with diabetes
Telmisartan has one more property that occasionally tips the decision: it behaves in a metabolically favorable way, with some studies suggesting a small beneficial effect on how the body handles blood sugar and fats. It’s not a diabetes drug, and no one prescribes it for that reason alone — but for a patient who has high blood pressure and type 2 diabetes, that neutral-to-favorable metabolic profile is a gentle argument in telmisartan’s column. Losartan is metabolically neutral too and perfectly appropriate here; this is a nudge, not a deciding blow. The honest takeaway is that neither drug will hurt your metabolic numbers, and telmisartan might help them a little — a minor bonus rather than a headline.
Where these two sit among all the ARBs
Telmisartan and losartan aren’t the only ARBs — valsartan, olmesartan, candesartan, and irbesartan round out the class, each with its own duration and evidence quirks. So why do these two dominate the conversation? Losartan because it was first and is exhaustively studied; telmisartan because it pairs a class-leading half-life with genuine outcome data. If your doctor mentions a third ARB, it’s usually for a specific reason — a particular kidney or heart indication, or simply what your insurance covers. The framework in this article still applies: ask about duration, outcome evidence, and any bonus effects that match your other conditions.
Side Effects and Safety
The reassuring news: as ARBs, both drugs are well tolerated, and both largely avoid the dry cough that plagues ACE inhibitors. Their side-effect profiles are more alike than different.
| Side effect | Telmisartan | Losartan | What to do |
|---|---|---|---|
| Dizziness / low BP | Occasional | Occasional | Rise slowly; report if persistent |
| High potassium | Possible | Possible | Periodic blood tests |
| Kidney function changes | Possible | Possible | Monitored with blood tests |
| Dry cough | Rare | Rare | Usually a reason people switch to ARBs |
| Uric acid | Neutral | Lowers it (can help gout) | A plus for some patients |
Both share the same important safety rules. Neither should be taken during pregnancy — ARBs can harm a developing baby, so anyone who is or may become pregnant needs an alternative and should tell their doctor. Both require occasional blood tests to check potassium and kidney function, especially when starting or changing dose. And both can interact with certain other medicines (including some diuretics and anti-inflammatories), which is why your pharmacist reviews your full list.
The one practical differentiator: losartan’s mild uric-acid-lowering effect. For a patient who has both high blood pressure and gout, that quirk can make losartan the tidier single-drug choice — one pill helping two problems.
A word on what to watch for regardless of which you take. Call your doctor if you develop swelling of the face, lips, or tongue (a rare reaction called angioedema), persistent dizziness or fainting, or signs of high potassium such as muscle weakness or an irregular heartbeat. These are uncommon, but they apply to the whole ARB class. Routine blood tests exist precisely to catch the quieter issues — potassium and kidney changes — before they cause symptoms, which is why keeping those follow-up appointments matters even when you feel completely fine.
Thinking about switching?
Switching between these two is common and usually straightforward, but it belongs to your prescriber, not to trial and error. A doctor switching you will choose a comparable dose, not simply swap the number — telmisartan 40 mg and losartan 50 mg are roughly in the same ballpark, but the exact equivalence depends on your readings. After a switch, expect a follow-up blood pressure check and, often, a blood test in a few weeks to confirm the new drug is doing its job without nudging your potassium or kidney numbers. The good news: because both are ARBs, moving between them rarely causes the abrupt problems that switching between entirely different drug classes sometimes does.
What Does the Research Say?
| Study | Year | Finding | Source |
|---|---|---|---|
| Ambulatory-BP meta-analysis | 2013 | Telmisartan lowered 24-h BP ~2.1/1.6 mmHg more than losartan; ~3.0/2.2 more in last 6 h | PMID 23945962 |
| Titration-to-response meta-analysis | 2003 | Telmisartan achieved greater BP response across titration | PMID 12900588 |
| ONTARGET | 2008 | Telmisartan non-inferior to ramipril for major CV events, better tolerated | PMID 18378519 |
What this means for you: the research consistently gives telmisartan a small efficacy edge for round-the-clock control and a unique cardiovascular-outcome credential. But “small edge” is the honest phrase — for many people with well-controlled pressure on losartan, there’s no compelling reason to switch. Evidence favors telmisartan on paper; your individual response, tolerance, and other conditions decide the real-world winner.
Who Should Choose Which
Let’s turn the evidence into a practical decision.
Telmisartan may suit you if:
- Your blood pressure runs high in the early morning or overnight.
- You’re at higher cardiovascular risk and want the ONTARGET-backed option.
- You occasionally miss a dose and want a more forgiving, long-acting drug.
- You want maximal 24-hour consistency from a single daily pill.
Losartan may suit you if:
- You also have gout or high uric acid (losartan’s bonus effect helps).
- You’re already well-controlled on it with no side effects — stability has value.
- Your clinician prefers it for a specific reason, such as certain kidney or heart-chamber indications where it has strong evidence.
- Cost or formulary coverage favors it (both are cheap, but plans differ).
If you’re navigating this decision later in life, where fall risk and multiple medications complicate everything, our guide to blood pressure medication for seniors is worth reading alongside this. And for the full landscape of options beyond ARBs, see our roundup of the best blood pressure medications. MedsBase stocks both drugs — telmisartan as Telma and losartan as Losar — so you can check availability once you and your doctor decide.
Related reading
Frequently Asked Questions
Is telmisartan better than losartan?
On paper, telmisartan has a small edge: a longer half-life, slightly stronger 24-hour blood pressure control, and unique cardiovascular-outcome evidence from the ONTARGET trial. But “better on average” isn’t “better for everyone.” If you’re well-controlled on losartan or benefit from its uric-acid-lowering effect, it may be the right drug for you.
What is the main difference between telmisartan and losartan?
Duration. Telmisartan’s half-life is about 24 hours, giving very consistent around-the-clock control, while losartan works largely through a shorter-lived active metabolite. Telmisartan also has ONTARGET cardiovascular-protection evidence; losartan has a mild uric-acid-lowering benefit.
Which ARB lasts the longest?
Telmisartan has one of the longest half-lives among ARBs, at roughly 24 hours. That’s why it tends to control blood pressure better in the last hours before the next dose — the overnight and early-morning window when cardiovascular risk is highest.
Can you switch from losartan to telmisartan?
Often yes, and it’s a common switch when a doctor wants stronger 24-hour control or added cardiovascular evidence. Any change should be made by your prescriber, who will pick an equivalent dose and monitor your blood pressure and blood tests afterward. Never switch on your own.
Do telmisartan and losartan have different side effects?
They’re broadly similar — both are well-tolerated ARBs that rarely cause the ACE-inhibitor cough. The notable difference is that losartan mildly lowers uric acid, which can help people with gout. Both require occasional blood tests and neither is safe during pregnancy.
Which is cheaper, telmisartan or losartan?
Both are available as inexpensive generics, so cost is rarely the deciding factor. Exact pricing depends on your pharmacy and insurance formulary. The clinical differences — duration and cardiovascular evidence versus the uric-acid benefit — usually matter more than the small price gap.
Can telmisartan or losartan be combined with other blood pressure drugs?
Yes — both are frequently paired with a diuretic (like hydrochlorothiazide) or a calcium channel blocker (like amlodipine), often in a single combination pill to simplify your routine. If one ARB at a full dose doesn’t get you to target, adding a second class is usually more effective and better tolerated than pushing the ARB dose higher. Your doctor decides the combination based on your readings and other conditions.
Is one safer for the kidneys?
Both ARBs can actually protect the kidneys in the right patients, particularly those with diabetes, and both require periodic blood tests to monitor kidney function and potassium. Neither is universally “safer” for kidneys — the right choice depends on your specific kidney status, which your doctor tracks over time. Anyone with significant kidney disease needs individualized advice.
The Bottom Line
In telmisartan vs losartan, telmisartan wins the spec sheet: longer half-life, steadier 24-hour control, and ONTARGET cardiovascular-protection evidence that few ARBs can match. That makes it a strong default for higher-risk patients and anyone whose pressure climbs before the next dose is due.
But losartan isn’t the runner-up so much as the right answer for a different person — someone stable on it, or someone whose gout benefits from its uric-acid effect. This is the resolution of the tension we opened with: telmisartan looks stronger and losartan stays popular because “strongest” and “best for you” are genuinely different questions.
Your immediate action: don’t switch on your own. If this comparison made you wonder whether you’re on the right ARB, bring it to your doctor or pharmacist with your blood pressure log — that conversation, backed by your actual numbers, is what turns a good comparison into the right prescription.
Managing cholesterol alongside your blood pressure? Our guide to the new oral PCSK9 inhibitor covers the other half of heart protection. Want the full menu of options? Start with the best blood pressure medications.
Medical Disclaimer
This article is for general education and is not medical advice. Choosing or switching blood pressure medication — including between telmisartan and losartan — should be done with your doctor or pharmacist based on your full health picture. Neither drug is safe in pregnancy. Never start, stop, or switch a prescription on your own.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.