







PCT Stack — Clomisign + Tamoxilon (Clomiphene + Tamoxifen)

PCT Stack — Clomisign 50 mg (clomiphene) + Tamoxilon 20 mg (tamoxifen) bundled. Classical SERM PCT to restart endogenous testosterone after exogenous androgen suppression. Standard 4-week protocol. Specialist-supervised use only.
✓ Medically reviewed by Morgan Ellis — Pharmacy Researcher · 8 years experience · Last reviewed: May 2026
Quick Answer — What is the PCT Stack?
The MedsBase PCT (Post-Cycle Therapy) Stack pairs clomiphene 50 mg (Clomisign by Signature) with tamoxifen 20 mg (Tamoxilon) — the two SERMs (selective oestrogen-receptor modulators) used for decades to restart endogenous testosterone production after exogenous androgen suppression of the HPGA. Standard 4-week PCT protocol following a typical anabolic cycle or after long-term TRT discontinuation. Supply tiers: 1, 3, or 6 months (1, 2–3, or 5–6 PCT cycles). Specialist-supervised use only.
📦 Every order is covered by our Reshipment Assurance Policy — if your parcel does not arrive within 20 business days, we reship it.
Why order from MedsBase
Our generic medications are sourced from WHO-GMP certified manufacturers and shipped worldwide in discreet, plain packaging — no medication name on the parcel exterior. Card payments are routed through a regulated processor (statement descriptors include a regulated card-payment processor — never “MedsBase” or any medication name). Crypto and SEPA bank transfer are also accepted. Every order is backed by our Reshipment Assurance Policy.
What’s in the PCT Stack
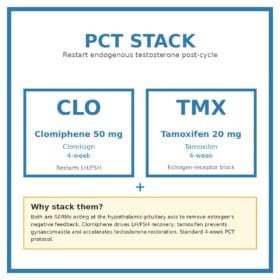
- Clomisign 50 mg (clomiphene citrate, Signature). Mixed oestrogen-receptor agonist/antagonist — antagonist at the hypothalamus (lifting GnRH suppression and triggering LH/FSH release), agonist at peripheral tissues. Restarts the testes’ endogenous testosterone production.
- Tamoxilon 20 mg (tamoxifen citrate). SERM with strong antagonist activity at breast tissue and the hypothalamus, mild agonist activity at bone and uterus. Adds to the LH/FSH-restart effect of clomiphene and protects against rebound oestrogen-driven gynaecomastia during the recovery window.
The clomiphene + tamoxifen combination is the classical “Nolva + Clomid” PCT pattern used in bodybuilding circles and supported by clinical literature on hypogonadism recovery (Katz et al. 2012, Tan et al. 2013). It is more aggressive than tamoxifen alone and faster-acting than clomiphene alone.
Why combine clomiphene and tamoxifen?
Suppression of the hypothalamic-pituitary-gonadal axis (HPGA) by exogenous androgens (testosterone esters, oral 17α-alkylated steroids, designer SARMs) produces a recovery window where endogenous LH and FSH are suppressed to near zero and serum testosterone may take 6 months or more to recover spontaneously. The recovery window is the highest-risk period for: persistent low-T symptoms (low libido, low mood, low energy, ED), gynaecomastia (oestrogen rebound from aromatising fat stores), and loss of any gains made during the cycle.
Clomiphene and tamoxifen attack the recovery from two angles: clomiphene drives the pituitary to release more LH (the dominant signal for testosterone restart), tamoxifen blocks the breast-tissue oestrogen receptor (preventing gynaecomastia regardless of oestrogen rebound). The pair shortens the recovery window from 4–6 months to roughly 4–6 weeks for most users.
Who this stack is for
Best candidates:
- Men coming off a 6–12 week anabolic-androgenic steroid cycle
- Men ending long-term TRT under medical supervision (with a goal to restore endogenous testosterone)
- Men who have used SARMs for 8+ weeks at suppressive doses
- Men with secondary hypogonadism (low LH/FSH with low testosterone) where SERM monotherapy is being considered as an alternative to TRT
NOT appropriate for:
- Women — clomiphene has fertility-induction uses in women under specialist supervision; off-label use otherwise risks ovarian hyperstimulation
- Anyone with active or prior breast cancer (tamoxifen is itself a breast-cancer treatment, but unsupervised use is dangerous)
- Anyone with a history of thromboembolic disease, recent MI/stroke — both SERMs raise VTE risk
- Anyone with severe hepatic impairment
- Men with primary hypogonadism (testicular failure with high LH) — SERMs cannot fix the testis
- Anyone unwilling to do baseline + post-PCT bloodwork (LH, FSH, total + free T, oestradiol, SHBG)
Standard PCT protocol
Start timing: 2–3 weeks after the last long-ester injection (test enanthate, test cypionate); 5–7 days after the last short-ester (test propionate); 3 days after the last oral. Starting too early while exogenous androgens are still suppressing the HPGA wastes the SERM dose.
| Week | Clomiphene | Tamoxifen |
|---|---|---|
| Week 1 | 50 mg twice daily | 40 mg once daily (2× tablets) |
| Week 2 | 50 mg once daily | 40 mg once daily |
| Week 3 | 50 mg once daily | 20 mg once daily |
| Week 4 | 25 mg once daily | 20 mg once daily |
This is the classical 4-week protocol. Some users extend tamoxifen by 1–2 weeks at 20 mg if oestradiol rebound symptoms persist. Bloodwork at week 6–8 post-PCT should show LH, FSH, total testosterone, free testosterone, and oestradiol returning to baseline.
Combined-use safety
Critical warning — VTE risk
Both clomiphene and tamoxifen raise the risk of venous thromboembolism (DVT, PE). The combined risk during PCT is small in healthy young men but is real. Do not stack with prolonged immobilisation, long-haul flights without prophylaxis, or known thrombophilia. Stop both drugs and seek emergency care for sudden unilateral leg swelling, chest pain, breathlessness, or signs of stroke.
Clomiphene’s mood effects are dose-related — at 50 mg twice daily in week 1 some users experience irritability, low mood, or visual disturbance (“clomid floaters”). The week-1 high dose can be reduced to 50 mg/day if tolerability is poor; recovery is slightly slower but more comfortable.
Tamoxifen does not affect IGF-1 the way clomiphene can blunt it. Combining the two does not blunt the IGF-1 spike from the testosterone recovery itself.
Bloodwork — what to test and when
| Test | When |
|---|---|
| Total + free testosterone, LH, FSH, oestradiol, SHBG, prolactin | Baseline before cycle; at start of PCT; 4 weeks post-PCT; 8 weeks post-PCT |
| Liver panel (ALT, AST, GGT, ALP, bilirubin) | Baseline; mid-cycle if oral steroids used; 2 weeks post-PCT |
| Lipid panel (TC, HDL, LDL, triglycerides) | Baseline; 4 weeks post-PCT |
| Full blood count (haematocrit, haemoglobin) | Baseline; mid-cycle |
Frequently Asked Questions
Is this the same as buying Clomisign and Tamoxilon separately?
Exactly the same products — Signature’s Clomisign 50 mg and Tamoxilon 20 mg, shipped together. The stack pricing is lower than buying each alone.
Why not include an aromatase inhibitor (AI) like anastrozole?
The classical SERM-only PCT was designed to allow oestradiol to rise during recovery, which is needed for libido, mood, and bone signalling. AIs crash oestradiol and can worsen recovery feel. AIs have a role for active gynaecomastia control during the cycle itself, not in PCT. If you need anastrozole, it is a different conversation.
Can I do PCT with tamoxifen alone?
Yes — tamoxifen 20 mg/day for 4 weeks is a milder PCT often used after short or low-dose cycles. The clomiphene + tamoxifen combination is more aggressive and faster, suited to longer or stronger cycles.
Can I do PCT with clomiphene alone?
Yes — but you lose the gynaecomastia protection that tamoxifen provides. Solo clomiphene is reasonable after a mild cycle in a man who has never had gyno symptoms.
When do I start PCT after my last injection?
Long-ester testosterone (enanthate, cypionate): 2–3 weeks after last injection. Short-ester (propionate): 5–7 days. Suspension: 24 hours. Orals (Dianabol, Anavar, etc.): 3 days. SARMs: 3 days. Trenbolone: 3 weeks. Nandrolone (Deca): 3–4 weeks (long ester clearance). Starting too early is the most common PCT mistake.
What does “clomid floaters” mean?
Visual disturbances — small bright spots or shimmer in peripheral vision — reported by ~5% of men on clomiphene at higher doses. Usually resolves on dose reduction; rare reports of persistent visual symptoms exist. Stop and consult a clinician if visual symptoms persist beyond a few days of stopping the drug.
Can I drink alcohol during PCT?
Moderate alcohol does not interact with the drugs but it raises oestradiol via aromatisation in fat tissue and slows the LH recovery you are trying to drive. Practical answer: minimise alcohol during the 4-week PCT for best recovery.
Will my libido return immediately?
Usually a partial return at the end of week 2 as LH/FSH rise; substantial return by week 6 post-PCT once the testosterone-oestradiol-SHBG balance restabilises. If you have no improvement in libido at 8 weeks post-PCT, get bloodwork — incomplete recovery happens, especially after long or repeat cycles.
Can I pay with cryptocurrency?
Yes — Bitcoin, Ethereum, USDT and other major cryptocurrencies via Plisio with an automatic 10% discount at checkout. See the Crypto Payment Guide.
How is the stack shipped?
Discreet plain packaging with no drug names on the outside. Worldwide delivery. The Reshipment Assurance Policy covers a free reship if your parcel does not arrive within 20 business days.
What you get in each tier
Each PCT “cycle” is a 4–6 week course. The 1-month tier covers one full PCT; the 3- and 6-month tiers cover three or six discrete PCT cycles for repeat users. Do not extend a single cycle beyond 6 weeks.
| Tier | Contents |
|---|---|
| 1 Month |
|
| 3 Months |
|
| 6 Months |
|
Also in our Hormonal Recovery range
- Clomiphene alone: Clomisign, Clomiford, Enclomisign (enclomiphene-only isomer)
- Tamoxifen alone: Tamoxilon, Tamodex, Tamilong
- Aromatase inhibitors (gyno control during cycle): Letroheal (letrozole), Fempro, Xtane (exemestane)
- HCG (testicular maintenance during cycle): HUCOG 5000IU Injection, Eutrig HP 5000IU Injection
- See the full Men’s Health category
Important safety information
Clomiphene and tamoxifen are specialist-supervised medicines and should be used under medical supervision. PCT is appropriate only after confirmed HPGA suppression from exogenous androgens. Do not use if you have active or prior breast cancer, history of venous thromboembolism (DVT/PE), recent stroke or MI, severe hepatic impairment, or known SERM hypersensitivity. Stop both drugs and seek emergency care for sudden unilateral leg swelling, chest pain, shortness of breath, slurred speech, weakness or numbness on one side (signs of stroke or VTE), persistent visual disturbance, or signs of severe hypersensitivity. This page is for educational purposes and does not replace consultation with a qualified clinician. Self-administered anabolic-androgenic steroid use carries significant cardiovascular, hepatic, fertility, and mental-health risks separate from the recovery phase.
More options in Men's Health
Ranked by recent MedsBase order volume — what other customers in this category are picking.



| Quantity | 1 Month, 3 Months, 6 Months |
|---|
 PCT Stack — Clomisign + Tamoxilon (Clomiphene + Tamoxifen)
PCT Stack — Clomisign + Tamoxilon (Clomiphene + Tamoxifen)
Q & A
PCT Stack — Clomisign + Tamoxilon (Clomiphene + Tamoxifen)
Related products























Reviews
There are no reviews yet