







✓ Medically reviewed by · Last reviewed: May 2026
Pharmacy Researcher · 8 years experience
Pharmacy researcher with 8 years reviewing clinical drug information, generic formulation equivalence, and international pharmaceutical standards. Focuses on patient-facing accuracy in medication education.
Key Takeaways
- There is no single best antiparasitic — the right drug depends on the parasite (worm, fluke, tapeworm, protozoan), the body site, and patient factors (pregnancy, age, co-infections).
- Ivermectin is the gold standard for onchocerciasis, strongyloidiasis, scabies, lice; safer than diethylcarbamazine in mixed-infection regions.
- Albendazole is the broadest-spectrum oral wormer — first-line for hookworm, ascariasis, trichuriasis, hydatid disease and as an MDA partner in lymphatic filariasis.
- Praziquantel is the only drug that reliably treats schistosomiasis and most tapeworms / flukes — every other antiparasitic misses these.
- Metronidazole / tinidazole handle protozoal infections (amoebiasis, giardiasis, trichomoniasis) — they do not kill worms.
- For mass drug administration (MDA) of lymphatic filariasis, the WHO standard is ivermectin + albendazole, OR diethylcarbamazine (DEC) + albendazole outside Africa where onchocerciasis overlap is rare.
Best Antiparasitic Medications & Combinations (2026): Worm, Fluke, Tapeworm & Protozoan Treatments
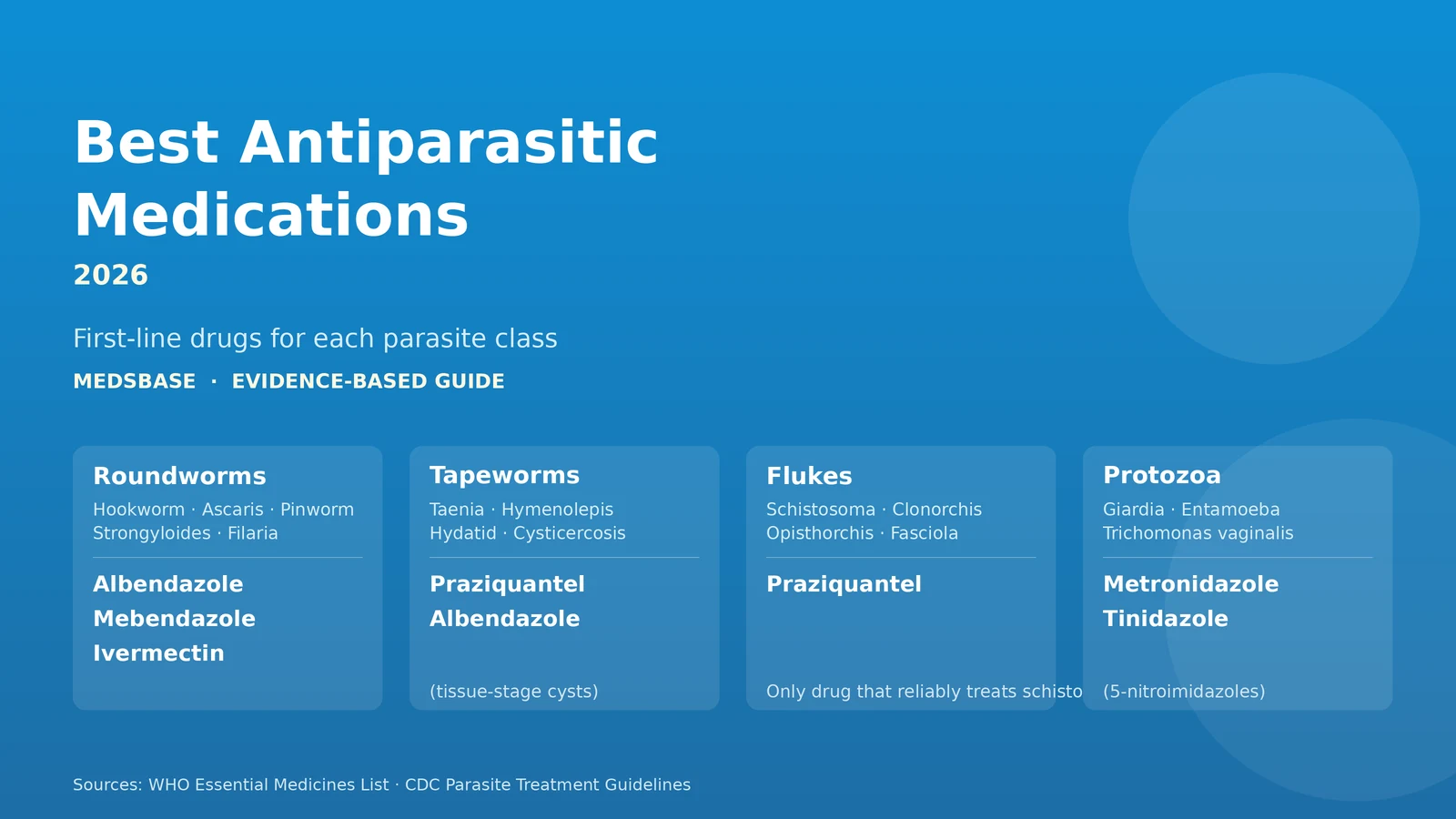
Parasitic infections cover four very different classes of organism — nematodes (round worms — hookworm, ascaris, pinworm, trichuris, strongyloides, filariae), cestodes (tapeworms — taenia, hymenolepis), trematodes (flukes — schistosoma, fasciola, opisthorchis), and protozoa (giardia, entamoeba, trichomonas, cryptosporidium). No single drug covers them all, and matching drug to parasite is the difference between cure and prolonged disease.
This guide covers the WHO-listed first-line antiparasitic drugs available at MedsBase, when each is used, what it costs, and which combinations matter — including the WHO mass-drug-administration (MDA) regimens used to eliminate lymphatic filariasis and the specific combinations that help in mixed parasite infections common in returning travellers and migrants from endemic regions.
Table of Contents
- How antiparasitics work — mechanism overview
- The 9 best antiparasitic medications and combinations (2026)
- Comparison table — at-a-glance
- Decision shortcut — pick by parasite
- Safety, contraindications and pregnancy
- Why combinations matter
- Frequently asked questions
- Bottom line
How antiparasitics work — quick mechanism overview
The major drug classes target different parasite biology — five mechanisms, five non-overlapping spectrums. The diagram below sets out the molecular target and what each class actually kills:
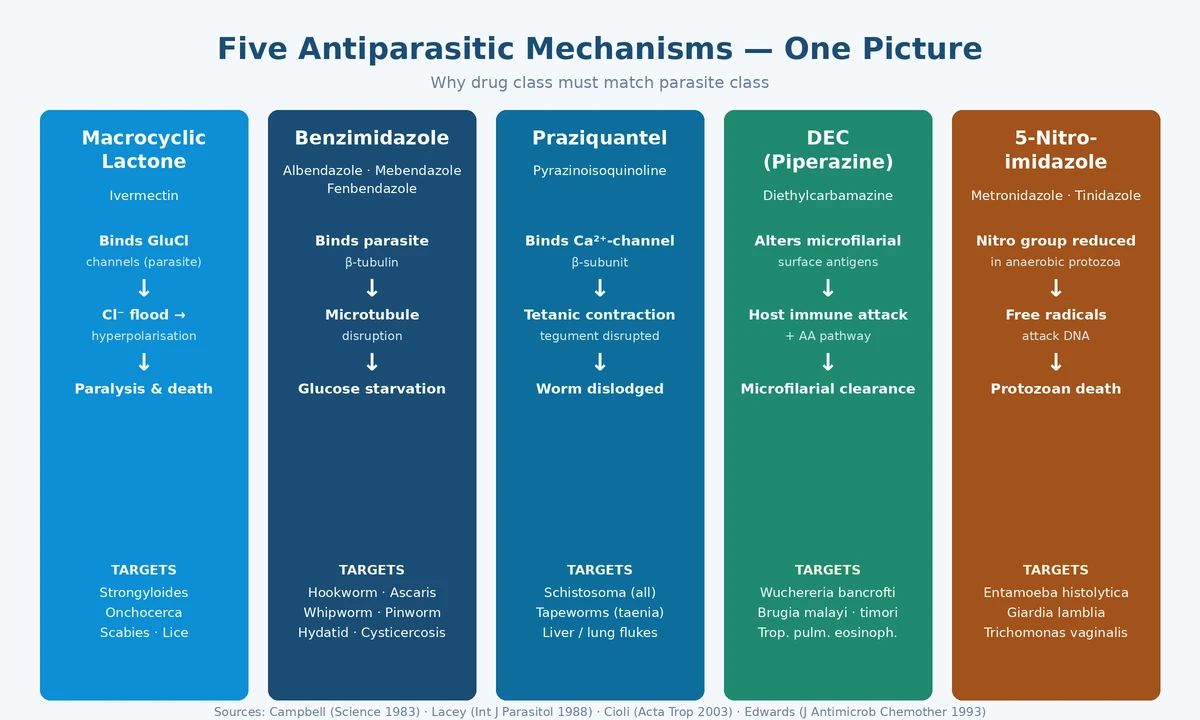
- Macrocyclic lactones (ivermectin) — open glutamate-gated chloride channels in invertebrate nerve and muscle cells, causing paralysis. Mammals lack these channels at relevant tissue exposures, hence the wide therapeutic margin.
- Benzimidazoles (albendazole, mebendazole, fenbendazole) — bind helminth β-tubulin, blocking microtubule polymerisation; the worm cannot maintain its gut, glucose uptake stops, the parasite starves over days.
- Praziquantel — induces tetanic muscular contraction and tegumental disintegration in flukes and tapeworms. Mechanism not fully understood; involves voltage-gated calcium channel β-subunit binding.
- Diethylcarbamazine (DEC) — sensitises microfilariae to host immune attack via altered surface antigens and arachidonic-acid pathway activation.
- 5-nitroimidazoles (metronidazole, tinidazole) — anaerobic protozoa reduce the nitro group to free radicals that damage parasite DNA. Aerobic mammalian cells do not reduce the drug significantly.
The 9 best antiparasitic medications and combinations (2026)
1. Ivermectin (Vermact, Ivecop, Ivecop DT) — gold-standard for onchocerciasis, strongyloidiasis, scabies
Single-dose 200 μg/kg orally clears strongyloides, scabies and onchocerciasis microfilariae. The Mectizan Donation Program has used ivermectin since 1987 to eliminate river blindness in Africa and Latin America. Also treats head lice, cutaneous larva migrans, and gnathostomiasis. Repeat dose at day 7–14 for scabies. Stocked formats: 6 mg / 12 mg standard tablet, 6 mg dispersible (DT) for paediatric or NG-tube administration.
2. Albendazole (ABD 400, Wormentel) — broadest-spectrum oral wormer
Single 400 mg dose clears hookworm, ascariasis (round worm), trichuriasis (whipworm) and pinworm. Extended courses (10 mg/kg/day for 8–30 days, often cycled) treat cystic echinococcosis (hydatid disease), cysticercosis and strongyloidiasis. Also the WHO MDA partner for lymphatic filariasis (with ivermectin or DEC). Take with fatty food for ×5 absorption when treating tissue helminths. (Wormentel is a fenbendazole brand sometimes co-listed here — see picks 9 and the fenbendazole vs ivermectin guide for the distinction.)
3. Mebendazole (Mebex) — first-line for pinworm and simple intestinal worms
Single 100 mg dose for pinworm; repeat at 2 weeks to catch newly hatched larvae from contaminated bedding/towels. 100 mg twice daily for 3 days for hookworm, ascariasis or trichuriasis. Less systemic absorption than albendazole — often preferred in children and where systemic exposure is a concern. Not effective for tissue helminths (use albendazole).
4. Diethylcarbamazine — DEC (Hetrazan) — antifilarial for lymphatic filariasis and TPE
WHO first-line for Wuchereria bancrofti, Brugia malayi, Brugia timori lymphatic filariasis and tropical pulmonary eosinophilia (TPE). Adult dose 6 mg/kg/day for 12 days, or single 6 mg/kg + albendazole 400 mg in MDA. Critical exclusion: in onchocerciasis (river blindness) DEC triggers severe Mazzotti reaction with irreversible eye damage — use ivermectin instead. In high-burden Loa loa it can cause fatal encephalopathy — pre-treatment microfilarial counting required.
5. Praziquantel (Prazihet, Prazinec) — schistosomiasis, tapeworms, flukes
The only drug that reliably treats schistosomiasis (all species — S. haematobium, S. mansoni, S. japonicum), tapeworm infections (Taenia saginata, T. solium intestinal, Hymenolepis nana, Diphyllobothrium latum) and liver/lung flukes (Clonorchis, Opisthorchis, Paragonimus, Fasciola — partial). Schistosomiasis dose 40–60 mg/kg single or split. Tapeworm dose 5–10 mg/kg single. Take with food for absorption.
6. Metronidazole (Metrogyl) — first-line for amoebiasis, giardiasis, trichomoniasis
The workhorse 5-nitroimidazole for protozoal infections. Amoebic dysentery: 500–750 mg three times daily for 7–10 days, followed by a luminal amoebicide (paromomycin or diloxanide). Giardiasis: 250 mg three times daily for 5–7 days. Trichomoniasis: 2 g single dose or 500 mg twice daily for 7 days; treat partner. Anaerobic bacteria too. Disulfiram-like reaction with alcohol — avoid all alcohol during course AND 48 hours after.
7. Tinidazole (Tiniba, Tinvista) — single-dose alternative to metronidazole
Newer 5-nitroimidazole with a longer half-life enabling single-dose regimens. Giardiasis: 2 g single dose (vs 5–7 days metronidazole). Trichomoniasis: 2 g single dose (treat partner). Amoebiasis: 2 g daily for 3 days. Better tolerated than metronidazole — less metallic taste, fewer GI effects. Same disulfiram-like alcohol interaction. The same luminal-amoebicide follow-up rule applies after invasive amoebiasis.
8. Ivermectin + Albendazole — WHO MDA combination for lymphatic filariasis
Taken together as ivermectin 200 μg/kg + albendazole 400 mg, single annual dose for 5–6 years to eliminate transmission. Used outside DEC-restricted regions (Africa where onchocerciasis overlap exists). The combination produces stronger and longer microfilarial suppression than either drug alone, and the partner activity hits incidental ascariasis, hookworm and trichuriasis common in the same populations. We supply both molecules — order Vermact + ABD 400 together for one dose.
9. Ivermectin + Fenbendazole Combo (Combo Pack) — extended-spectrum protocol
A fixed combination of ivermectin and fenbendazole sold for veterinary deworming and increasingly explored in the alternative cancer-protocol literature (Joe Tippens protocol). Both are benzimidazole-class or macrolide-class antiparasitics with overlapping helminth coverage. Important: human cancer evidence is anecdotal — controlled trials are limited. We supply this combination but do not make therapeutic claims beyond the conventional antiparasitic indications. See the dedicated Joe Tippens Protocol guide for current evidence.
Comparison table — at-a-glance
| Drug | Class | Best for | Adult dose | Pregnancy |
|---|---|---|---|---|
| Ivermectin | Macrocyclic lactone | Strongyloidiasis, onchocerciasis, scabies, lice, gnathostomiasis | 200 μg/kg single (repeat at 14 d for scabies) | Avoid 1st trimester; OK 2nd–3rd if needed |
| Albendazole | Benzimidazole | Hookworm, ascariasis, trichuriasis, hydatid, cysticercosis, MDA partner | 400 mg single (intestinal); 10 mg/kg/day cycled (tissue) | Avoid 1st trimester |
| Mebendazole | Benzimidazole | Pinworm, simple intestinal worms (preferred in children) | 100 mg single, repeat 14 d (pinworm); 100 mg BID × 3 d (other) | Avoid 1st trimester |
| DEC (Hetrazan) | Piperazine | Lymphatic filariasis (Wuchereria, Brugia), TPE | 6 mg/kg/day × 12 d, or 6 mg/kg + ABZ single in MDA | Defer treatment |
| Praziquantel | Praziquantel | Schistosomiasis, tapeworms, flukes | 40–60 mg/kg single (schisto); 5–10 mg/kg single (tapeworm) | Compatible — schistosomiasis treated in pregnancy |
| Metronidazole | 5-Nitroimidazole | Amoebiasis, giardiasis, trichomoniasis, anaerobes | 500–750 mg TID × 7–10 d (amoebic), 2 g single (trich) | Avoid 1st trimester |
| Tinidazole | 5-Nitroimidazole | Single-dose giardiasis, trichomoniasis, amoebic abscess | 2 g single (giardia, trich); 2 g/d × 3 d (amoeba) | Avoid 1st trimester |
| Iverm + ABZ MDA | Combination | WHO lymphatic filariasis MDA outside Africa | Annual single dose × 5–6 years | Defer in pregnancy |
| Iverm + Fenben combo | Combination | Broad-spectrum deworming; off-label cancer-protocol use | Per protocol — see dedicated guide | Avoid 1st trimester |
Decision shortcut — pick by parasite
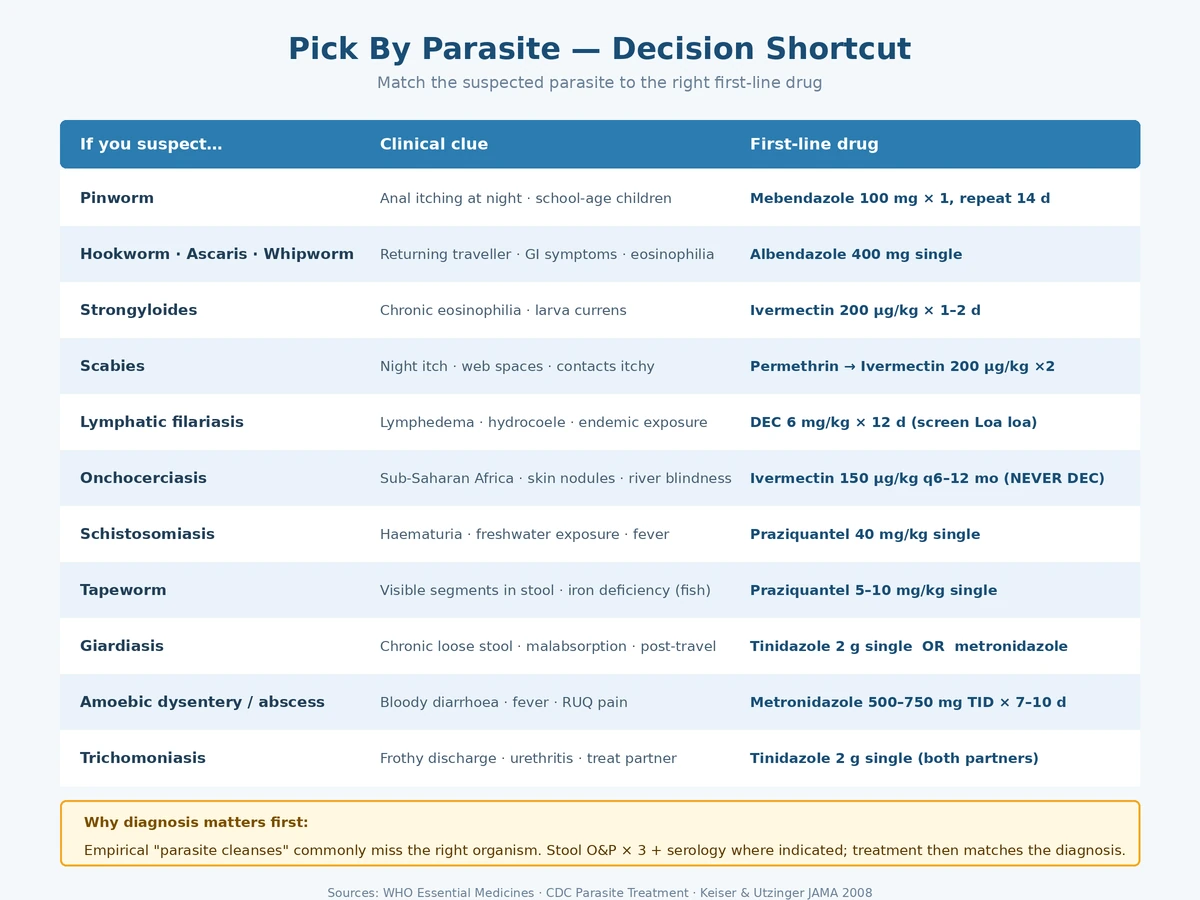
If you already have a likely parasite in mind (or a positive stool / serology test), use the table below to land on the right first-line drug at a glance. The detailed indication notes and dosing live in the picks above and in the comparison table.
If you suspect…
- Pinworm (anal itching especially at night, school-age children) → Mebendazole 100 mg single, repeat at 2 weeks; treat household.
- Hookworm, roundworm, whipworm (returning traveller, abdominal symptoms) → Albendazole 400 mg single.
- Strongyloidiasis (chronic eosinophilia, larva currens, hyperinfection risk in immunosuppressed) → Ivermectin 200 μg/kg × 1–2 days.
- Scabies (intense night itching, web spaces, household contacts itchy) → topical permethrin first-line; oral ivermectin 200 μg/kg at days 0 and 14 for resistant cases.
- Lymphatic filariasis (lymphedema, hydrocoele, endemic-area exposure, eosinophilia + microfilariae) → Hetrazan 6 mg/kg/day × 12 d, screen first for Loa loa and onchocerciasis.
- Onchocerciasis (river blindness, sub-Saharan Africa, skin nodules, papular dermatitis) → Ivermectin 150 μg/kg every 6–12 months. Never DEC.
- Schistosomiasis (haematuria, freshwater exposure in endemic Africa or Asia) → Praziquantel 40 mg/kg single.
- Tapeworm (segments in stool) → Praziquantel 5–10 mg/kg single.
- Giardiasis (chronic loose stool, malabsorption, post-travel) → Tinidazole 2 g single OR metronidazole 250 mg TID × 5–7 d.
- Amoebic dysentery / liver abscess (bloody diarrhoea, fever, RUQ pain) → Metronidazole 500–750 mg TID × 7–10 d followed by a luminal amoebicide.
- Trichomoniasis (frothy vaginal discharge, urethritis) → Tinidazole 2 g single for both partners.
Safety, contraindications and special populations
- Pregnancy — first-trimester avoidance is the rule for benzimidazoles (albendazole, mebendazole) and 5-nitroimidazoles (metronidazole, tinidazole). Praziquantel is considered compatible and is used to treat schistosomiasis in pregnancy. Ivermectin first-trimester data are limited; second-third trimester use is acceptable when needed. Diethylcarbamazine treatment is usually deferred.
- Loa loa screening — patients from Central Africa with eosinophilia need a daytime blood-film microfilarial count BEFORE ivermectin or DEC — high-density Loa loa + ivermectin can trigger fatal encephalopathy.
- Mazzotti reaction — DEC in onchocerciasis or ivermectin in heavy onchocerca burden produces fever, pruritus, lymphadenopathy as microfilariae die; manage with paracetamol and antihistamine. Severe cases need oral steroid.
- Children — most antiparasitics are safe over age 2 (some over 1). Use weight-based dosing and dispersible tablets where available (Ivecop DT).
- Drug interactions — albendazole + dexamethasone or cimetidine raises albendazole sulfoxide levels (relevant for tissue helminths). Metronidazole + warfarin = increased INR. Tinidazole + alcohol + 48 h after = disulfiram-like reaction.
Why combinations matter
The single biggest reason antiparasitic treatment fails is single-drug therapy in a multi-organism infection. Returning travellers from endemic regions commonly carry more than one parasite. Mass drug administration programs use combinations precisely because they:
- Suppress microfilariae more durably — ivermectin + albendazole produces longer-lasting microfilarial clearance than either drug alone in lymphatic filariasis (Tisch 2008 meta-analysis).
- Cover incidental co-infections — ascariasis, hookworm, trichuriasis are common where filariasis is endemic; the albendazole partner kills these incidentally.
- Reduce resistance pressure — single-drug MDA accelerates emergence of resistant subpopulations; combinations slow that.
- Improve community-level transmission interruption — the WHO Global Programme to Eliminate Lymphatic Filariasis credits the combination protocol for reducing global lymphatic filariasis prevalence by ~74% since 2000.
Frequently Asked Questions
Which antiparasitic kills the most parasite types?
None covers everything. Albendazole has the broadest single-agent spectrum across nematodes, larval cestodes (cysticercosis, hydatid) and as an MDA partner — but it does not treat schistosomiasis, fluke infections, or any protozoal infection. The closest practical "broad sweep" is the combination of ivermectin + albendazole + praziquantel, which together cover roughly 95% of clinically significant helminths.
How do I know I actually have a parasite vs IBS or food sensitivity?
The only reliable diagnosis is laboratory: stool ova-and-parasite microscopy (×3 specimens spaced 2–3 days apart), antigen tests (Giardia, Entamoeba, Cryptosporidium), serology (Strongyloides, Schistosoma) or sometimes endoscopy/colonoscopy for adult worms. Empirical "parasite cleanses" without testing are common but rarely justified — see our parasite cleanse evidence guide for a balanced view.
Can I take ivermectin and albendazole together at home?
Yes — this is the WHO MDA combination, well-tolerated, with extensive safety data at standard doses (ivermectin 200 μg/kg + albendazole 400 mg, single dose). It is not a routine self-treatment in non-endemic regions; in endemic regions or for documented mixed infection, it is the standard approach.
How is ivermectin different from fenbendazole?
Different drug classes. Ivermectin is a macrocyclic lactone (chloride channel opener); fenbendazole is a benzimidazole (microtubule binder, like albendazole and mebendazole). Both are antiparasitic but they hit different molecular targets. They are sometimes combined for broader spectrum and for the off-label cancer protocols. See our Fenbendazole vs Ivermectin guide for the detailed comparison.
Why does my doctor want me to take a second dose two weeks later?
Pinworm, scabies and many helminth infections have eggs or larvae that hatch after the first dose has cleared. The 2-week repeat catches the second generation before they reach sexual maturity. Skipping it is the most common reason "the worms came back" — they did not come back; they were never killed.
Is metronidazole an antibiotic or an antiparasitic?
Both. Metronidazole and tinidazole are 5-nitroimidazoles active against anaerobic bacteria (Bacteroides, Clostridium difficile, Helicobacter pylori as part of triple therapy) AND anaerobic protozoa (Entamoeba, Giardia, Trichomonas). Same mechanism: nitro-group reduction in low-oxygen environments produces DNA-damaging radicals.
What about the "parasite cleanse" herbal products at health stores?
Wormwood, black walnut hull and clove combinations have weak in-vitro evidence and almost no controlled human trial data. They are not equivalent to pharmaceutical antiparasitics. If you have a documented parasitic infection, evidence-based therapy is dramatically more effective. If you have non-specific GI symptoms without a positive stool test, parasites are unlikely to be the cause.
Can I prevent parasitic infections during travel?
Mostly through behaviour, not drugs: drink only sealed bottled / boiled water, avoid raw vegetables/salads in high-risk regions, avoid freshwater swimming in schistosomiasis-endemic areas, use deet/icaridin against insect-borne parasites, do not walk barefoot on soil where hookworm is endemic. Ivermectin or albendazole prophylaxis is not routinely recommended for short trips; mass drug administration is a public-health programme, not personal prophylaxis.
Bottom line
The right antiparasitic is the one matched to your specific parasite and clinical situation. For most simple intestinal worm infections in non-endemic settings, single-dose mebendazole or albendazole is enough. For chronic eosinophilia, post-travel diarrhoea or suspected systemic infection, get the parasite identified first — empirical treatment misses the diagnosis and may pick the wrong drug.
If you are in or returning from an endemic region with multiple risk exposures, the ivermectin + albendazole MDA combination has the strongest evidence and broadest practical coverage. For schistosomiasis, tapeworm or fluke infection, only praziquantel works. For protozoal disease (giardia, amoeba, trichomoniasis), the 5-nitroimidazoles (metronidazole or tinidazole) are first-line.
Browse the full Antiparasitic & Worm Treatments category for product details, prices and combinations.
Medical Disclaimer
This guide is for educational purposes only and is not a substitute for medical advice or laboratory diagnosis. Antiparasitic treatment should be matched to a specific diagnosed organism. Consult a qualified healthcare professional, especially before starting therapy in pregnancy, in immunosuppressed patients, in children under 2, or when multiple parasites are suspected.
Written by
Sophie ChenPharmaceutical Content Researcher · 8 years experience
Sophie Chen is a pharmaceutical content researcher with 8 years covering generic medication access and clinical pharmacology. She specialises in international regulatory frameworks, bioequivalence standards, and patient-facing education on therapeutic drug classes. She is not a clinician.